- 410 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
International Review of Experimental Pathology, Volume 30, is organized around the theme of renal disease. The choice of renal disease reflects both the author's personal interest and the realization that there is a need for such a collection of reviews in this area. There are many new books on renal pathology, but almost all have a clinical rather than experimental orientation. The book opens with a chapter on the pathogenesis of experimentally induced renal papillary necrosis and upper urothelial carcinoma. Subsequent chapters deal with the use of cell cultures in the study of renal diseases; mechanisms of cyclosporine nephrotoxicity in humans and animal systems; spontaneously occurring renal diseases in laboratory animals; and the use of video microscopy to define the reactivity of the renal microvasculature and the hydraulic permeability of the glomerular capillaries. This book will be of interest to a diverse group of readers interested in renal disease. This broad spectrum of potential readership is reflected in the list of contributors which includes, in addition to pathologists, nephrologists, anatomists, veterinarians, and experimental chemists. This volume will also be of interest to transplant surgeons and to pediatricians specializing in renal disease.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MédecineSubtopic
Médecine cliniqueExperimentally Induced Renal Papillary Necrosis and Upper Urothelial Carcinoma
PETER H. BACH and NEILL J. GREGG, Nephrotoxicity Research Group, Toxicology Unit, Robens Institute of Industrial and Environmental Health and Safety, University of Surrey, Surrey, Guildford GU2 5XH, England
Publisher Summary
This chapter discusses experimentally induced renal papillary necrosis and upper urothelial carcinoma. It presents several morphological, histochemical, and functional data to support several distinct series of pathological changes following the administration of 2-bromoethanamine (BEA). The earliest histochemical changes take place in the medullary matrix that appears to undergo depolymerization. The renal medullary interstitial cells are the first cell type to undergo degenerative change that is rapidly followed by damage to the delicate elements of the medulla. The collecting ducts and endothelial changes are late and generally follow the necrosis of other anatomical regions of the medulla. At present, the lipid changes in the medulla are not well understood, but they are similar to those already reported in human analgesic abusers. The early subtle degenerative changes in the proximal tubule do not appear to be central to the development of the papillary lesion, but the subsequent exfoliation of the brush border and proximal tubular cells are important components of the protein casts that begin to form in the distal nephron. These subsequently appear to play at least some role in the development of functional changes that cause marked proximal tubular dilatation. The chapter illustrates the time course of the major pathophysiological changes associated with the development of RPN, and its secondary consequences of cortical degeneration and upper urothelial hyperplasia.
I Introduction
The etiology of renal papillary necrosis (RPN) in humans has been associated with the long-term abuse of analgesics and therapeutic doses of nonsteroidal antiinflammatory drugs (NSAID). However, the lesion has not been clearly defined in terms of the exact causative agent(s), how much (of each) was taken to cause a lesion, and over what period. The primary pathogenesis and the role of other complicating factors are also not clearly understood, nor have the secondary pathophysiological consequences of RPN been adequately interrelated, despite the fact that chronic renal failure and upper urothelial carcinoma are frequently associated with analgesic abuse (Bach and Bridges, 1985).
The understanding of the pathophysiology of a chronically developing renal lesion in humans is a major problem in those conditions where the etiology has been clearly defined, because of the strong likelihood of concurrent and complicating secondary (and unrelated disease) factors. There are important anatomical and functional differences between the kidneys of most animals and humans (Mudge, 1982; Stolte and Alt, 1980). The use of experimental models has generally shown a number of very important clinical and morphological differences; therefore, the use of these models has often limited the understanding of similar conditions in humans.
Although RPN (and upper urothelial carcinoma) are examples of renal disease developing chronically in humans, it has been possible to study a number of chemicals that induce these lesions rapidly in experimental animals. These models (Bach and Hardy, 1985; Bach and Bridges, 1985) all have the important pathophysiological hallmarks of the lesion that has been described in humans (Burry, 1968; Burry et al., 1977; Rosner, 1976; Bach and Bridges, 1985). The use of these experimental models has therefore fortuitously provided a way to study the development of papillary necrosis and the progression to a series of renal changes similar to those seen in human analgesic abusers. These models are also allowing the interrelationship between the primary lesion and its secondary consequences to be defined in terms of biochemical mechanisms. An understanding of the molecular genesis of this syndrome may be highly relevant to improved clinical management of RPN and upper urothelial carcinoma in humans.
II Renal Papillary Necrosis and Upper Urothelial Carcinoma in Humans
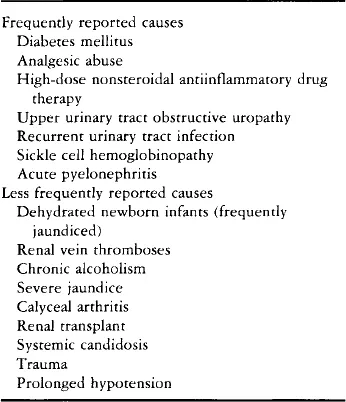
RPN was first described over 100 years ago (Turner, 1885). It is a lesion that may have a number of different causes (Table I), but most often when encountered in the clinical environment before the 1950s, was due to diabetes mellitus or sickle cell disease (Mandel, 1952). The most frequent cause of RPN since then (and in current clinical experience) is chronic, inappropriate, high-dose analgesic intake, especially the addiction to mixed analgesics over a number of years. Therapeutic closes of NSAID may also induce RPN (Nanra and Kincaid-Smith, 1972; Burry et al., 1977; Prescott, 1979, 1982; Bach and Bridges, 1985).
TABLE I
CAUSES OF RENAL PAPILLARY NECROSIS IN HUMANS
Initially, all of the mixed analgesics that were associated with the pyelonephritis seen in urology clinics contained phenacetin, and the condition was dubbed “phenacetin kidney” (Spuhler and Zollinger, 1953). Subsequently, however, it become apparent that other analgesics had the potential to cause RPN (Gilman, 1964). The early confusion over the cause of RPN, and the fact that most patients abused, or were prescribed, mixed analgesics and/or a number of different NSAID, also served to obscure case history data that might have provided vital information for the more accurate identification of which analgesics and/or NSAID had the greatest potential to cause the lesion (Cove-Smith and Knapp, 1978; Nanra and Kincaid-Smith, 1975; Nanra et al., 1980). The early failure to realize that phenacetin was not the sole cause of RPN shaped the dogma that resulted in the withdrawal of this drug from the market (Shelley, 1967, 1978). This, it was assumed, would remove the major etiological factor in the genesis of the lesion. When acetaminophen (paracetamol) replaced phenacetin in mixed analgesic preparations the incidence of RPN was expected to drop (Gault et al., 1968; Duggin, 1977; Kincaid-Smith, 1979). The occurrence of the lesion did not, however, decrease in those circumstances where the abuse of mixed analgesics continued (Prescott, 1979, 1982), although some decreases have been attributed to the withdrawal of phenacetin and extensive educational programs to discourage the abuse of mixed analgesics (Wilson and Gault, 1982). A variety of indirect evidence (Table II...
Table of contents
- Cover image
- Title page
- Table of Contents
- EDITORIAL ADVISORY BOARD
- Copyright
- Preface
- Chapter 1: Experimentally Induced Renal Papillary Necrosis and Upper Urothelial Carcinoma
- Chapter 2: The Contribution of Cell Culture to the Study of Renal Diseases
- Chapter 3: Cyclosporine Nephrotoxicity
- Chapter 4: Glomerular Antigens in Experimental Glomerulonephritis
- Chapter 5: Spontaneous Renal Disease in Laboratory Animals
- Chapter 6: The Use of Video Imaging Techniques to Study Ultrafiltration and Blood Flow in the Normal and Diseased Kidney
- Chapter 7: Chemically Induced Renal Epithelial Neoplasia in Experimental Animals
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access International Review of Experimental Pathology by G. W. Richter in PDF and/or ePUB format, as well as other popular books in Médecine & Médecine clinique. We have over 1.5 million books available in our catalogue for you to explore.