eBook - ePub
Health of HIV Infected People
Food, Nutrition and Lifestyle without Antiretroviral Drugs
- 420 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Health of HIV Infected People
Food, Nutrition and Lifestyle without Antiretroviral Drugs
About this book
Health of HIV Infected People: Food, Nutrition and Lifestyle Without Antiretroviral Drugs defines the supportive roles of bioactive foods, exercise, and dietary supplements on the health of HIV infected people who do not have access to resources or those who choose not to utilize antiretroviral drugs.
Approaches such as the application of traditional herbs and foods are given careful definition by experts who define the risks and benefits of such practices within this important context.
Readers learn how to treat or ameliorate the effects of chronic retroviral disease using readily available, cheap foods, and dietary supplements. Ultimately, this work delivers a current, concise, scientific appraisal of the efficacy of key foods, nutrients, dietary plants, and behavioral changes in preventing and improving the quality of life of HIV infected infants and adults who are not undergoing antiretroviral therapy.
- Covers the role of nutrients in the prevention and treatment of HIV-induced physiological changes
- Delivers important coverage on the relationship between HIV infection and infant feeding practice, along with public health policy recommendations in social and cultural context
- Provides coverage of fitness and exercise regimens, physical activity, and behavioral and lifestyle changes on HIV infected individuals
- Explores food and treatment of obesity, diabetes, and cardiovascular disease in HIV infected patients, including those without antiretroviral therapeutic treatmen
Information
Topic
MedicineSubtopic
AIDS & HIVSection II
Nutrition and Lifestyle
Outline
Chapter 6
Nutritional Treatment Approach for ART-Naïve HIV-Infected Children
Marianne de Oliveira Falco1 and Erika Aparecida da Silveira2, 1Department of Nutrition, Society Intensive Care, Goiás, Brazil, Postgraduate Studies Program Ph. D. in Health Sciences, Medical School, Federal University of Goiás, GO, Brazil, 2Researcher, teacher of Postgraduate Studies Program in Health Sciences, Department of Surgery, Medical School, Federal University of Goiás, GO, Brazil
Currently, 90% of children with human immunodeficiency virus (HIV) live in areas of food insecurity. Depletion of the immune system is caused by inadequate nutritional status, opportunistic infections, and HIV disease progression. Breastfeeding is one approach for minimizing frequent and numerous morbidities, and it should be encouraged even in areas of food insecurity and regions where access to ART is scarce. To facilitate proper treatment of malnutrition or weaning, some formulas are used alone or in addition to daily intake. Vitamins, minerals, and trace elements supplementation are also common strategies for nutritional status recovery, prevention, and treatment of morbidity and immune function improvement. There have been attempts to advance the reproduction of the benefits of breast milk via supplementation with probiotics. Nutritional treatment is the major agent for helping HIV-infected children who exhibit dietary deficiencies.
Keywords
HIV; children; malnutrition; breastfeeding; complementary feeding; micronutrients; probiotics
6.1 Introduction
There are currently 3.3 million children up to 14 years old living with human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) worldwide, with two-thirds in sub-Saharan Africa [1,2]. Sub-Saharan Africa, along with Asian countries, is an area with the second largest occurrence of infected children [1]. Besides the high prevalence of HIV infection, it is also a region of food insecurity [3].
Food insecurity and HIV infection are major triggers of dietary deficiencies and malnutrition [3]. Malnutrition in areas of food insecurity affects 18–47% of children infected with HIV [4,5].
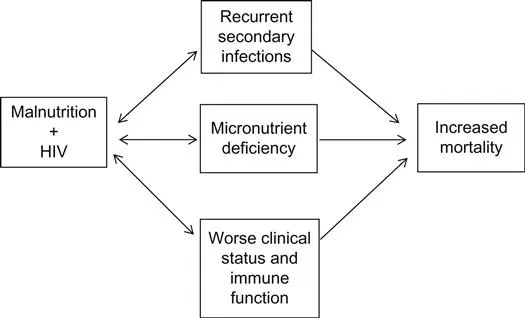
Immune system impairment, anemia, and malnutrition are the top three causes of HIV disease progression [2,6–10]. In HIV-infected children, malnutrition is associated with complications such as opportunistic infections, disabsorptive diseases, fluid and electrolyte disorders, and micronutrient deficiencies, which contribute to a significant increase in mortality, reaching 30% among hospitalized malnourished children [11,12]. These complications impair nutritional status, generating a vicious cycle (Figure 6.1) [13–15].
Given this framework, international organizations propose that 50% of HIV treatment is nutritional treatment and 50% is medical care [10,16].
6.1.1 Proposals and Investigations About Nutritional Approach for HIV-Infected Children
Proposals and research on the nutritional approach in HIV-infected children are guided by consolidated actions and often have positive outcomes. For example, supplementation with micronutrients, such as vitamin A, zinc, and iron, along with breastfeeding have provided encouraging evidence of improvement in morbidity and mortality in uninfected malnourished children [17–19]. These recommended approaches, widely disseminated since 2003 by the World Health Organization (WHO), are exposed, compared, and discussed along with other proposals in this chapter [20].
6.2 Nutritional Treatment and Ready-to-Use Formulas
6.2.1 Breastfeeding
Breast milk is the best and most complete food for infants. It helps prevent malnutrition, diarrhea, and recurrent infections. Therefore, it is an important immunomodulatory factor in the presence of HIV [7,16].
Children from 6 to 11 months who are exposed to HIV and who were not breastfed are at increased risk for hospitalization and have higher incidences of fever, diarrhea, and severe malnutrition [21]. In areas where ART is available, such as Brazil, North America, Europe, East Mediterranean region, and the Western Pacific [22], HIV-infected mothers should be strongly encouraged to breastfeed for 12 months or at least for a minimum of 6 months. Where ART is not available, the recommendation is the same because the protective effect of breastfeeding against morbidities arising from HIV infection is greater than the risk of HIV transmission during breastfeeding [16].
Not breastfeeding implies a survival risk for the child, especially in areas where there is food insecurity [22,23]. Its replacement with artificial feeding should only occur when there is an agreement between the mother and the health care professional that it is safe, feasible, affordable, and sustainable [16].
6.2.2 Weaning and Complementary Feeding
The weaning process, with the introduction of new foods, exposes HIV-infected children to the risk of malnutrition and other diseases, especially in areas of food insecurity, low income, and inadequate sanitation [7,16]. Early weaning increases rates of diarrhea and mortality, especially in malnourished children, compared with children who had long-term breastfeeding [7].
For the treatment and control of malnutrition, complementary foods, easy acquisition formulas, or preparation formulas are recommended. For severely malnourished children and HIV-positive children, the same formulas composed of milk, oil, sugar and a mix of vitamins and minerals are indicated [7]. F-75 formula, used as a first early treatment of severe malnutrition, has low osmolarity, avoiding severe metabolic and electrolyte imbalances of the refeeding syndrome. F-100 formula, used in the rehabilitation phase, has a higher caloric density and higher osmolarity.
Health professionals prescribed the formulas according to nutritional status and clinical status to achieve 1.0–1.2 kcal/kg, 13% protein, and approximately 30–40% lipids. For micronutrient deficiencies, depending on the composition and quantity of complementary foods offered to children, supplementation with multivitamins and minerals is required [7,24,25]. The formulas prescribed are low-cost, are composed of local food, and are much more accessible than the industrial formulas. They are distributed by treatment centers or delivered to homes by health workers who actively search out malnourished children, and they can even be commercially acquired [25].
In a detailed analysis conducted by the authors of this chapter, many industrialized formulas have higher protein concentrations than observed in those recommended by the WHO (approximately 14–20% of the nutritional composition). Studies reporting some advantage of industrialized formulas instead of the F-75 and F-100 formulas were not found. Nevertheless, it is known that HIV infection increases energy expenditure and, consequently, protein requirements [26–28]. Besides the aforementioned formulas, there are other variations that are described in this chapter.
Because of the high prevalence of malnutrition and its comorbidities, a study in South Africa has proposed implementing an intensification program to treat malnutrition in the region’s hospitals and to assess what ready-to-use formulas are more commonly prescribed. The study included children aged younger than 1 year and those aged between 1 and 5 years. The program involved nutritionists training to better-identify symptoms of malnutrition, such as diarrhea, vomiting, and edema, encouraging breastfeeding and formula prescriptions for children according to malnutrition severity and clinical status. Of the children without diarrhea, 16% used supplemental formula F-75 and the other 84% used industrialized formulas similar to breast milk. Of those with diarrhea, 14% used F-75 and 86% used formulas similar to human milk; the most used formula was soy protein–based, with no lactose. In children without diarrhea, the most commonly used formulas were those acidified with a protein compound based on whey protein, which is similar to breast milk [29]. In this study, the most prescribed formulas for malnutrition in the absence or presence of diarrhea were industrialized. This finding contrasts with the 2013 WHO indication for treating malnutrition in areas of food insecurity (use of F-75 and F-100) [19].
Regarding the use of supplementary food to treat malnutrition, a study conducted with children exposed to HIV in Malawi assessed the acceptability of weaning among mothers, adherence to use of formula, and possible food intolerances in children. The food supplement substitute for breast milk was composed of peanut butter, soy milk powder, sugar, soy oil, soy protein, and a mixture of 22 vitamins and minerals. In each 100 g, there were 15 g of protein and 550 kcal. The food supplement was provided at the beginning of the weaning process, week 24 until week 48, starting with 75 g/day and increasing to 100 g/day. According to mothers’ self-report, 91% of children were successfully weaned and 18% had side effects such as diarrhea, vomiting, and const...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- Preface
- List of Contributors
- Acknowledgement
- Section I: Overview and Food
- Section II: Nutrition and Lifestyle
- Section III: Exercise and Behavioral Lifestyle Changes in the Prevention and Treatment of HIV/AIDS Nutritional Changes
- Section IV: Models of HIV: Lessons to be Learned from Animal Viruses
- Index
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Health of HIV Infected People by Ronald Ross Watson in PDF and/or ePUB format, as well as other popular books in Medicine & AIDS & HIV. We have over 1.5 million books available in our catalogue for you to explore.