- 436 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
The Vaccine Book
About this book
The Vaccine Book provides comprehensive information on the current and future world of vaccines. It reveals the scientific opportunities and potential impact of vaccines, including economic and ethical challenges, problems encountered when producing vaccines, how clinical vaccine trials are designed, and how to introduce vaccines into widespread use. Although vaccines are now available for many diseases, there are still challenges ahead for major diseases such as AIDS, tuberculosis, and malaria. The Vaccine Book is designed for students, researchers, public health officials, and all others interested in increasing their understanding of vaccines.Topics unique to this book:* Ethics * Economics * Diseases that could be prevented* Clinical trial designs* Ideas about the future of vaccines* Challenges facing research scientists in the vaccine area* Burden of vaccine-preventable illness and the impact of vaccines* Scientific obstacles to be overcome by existing and new vaccines* Basic mechanisms of host immunity and pathogen interaction with host tissues* New approaches to future vaccines against challenging diseases* Real and perceived safety issues which dominate vaccine development and vaccination policies* Microbial pathogenesis as a basis for vaccine design* Planning vaccine trials* Introducing new vaccines into the healthcare system * Future challenges for vaccines and immunizations
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
Epidemiology1
GLOBAL BURDEN OF DISEASE
PART A. The Burden of Vaccine-Preventable Diseases
MAUREEN BIRMINGHAM* and CLAUDIA STEIN†, *Vaccine Assessment and Monitoring, Department of Vaccines and Biologicals, World Health Organization, 1211 Geneva 27, Switzerland; †Epidemiology and Burden of Disease, Global Programme on Evidence for Health Policy, World Health Organization, 1211Geneva 27, Switzerland
I. INTRODUCTION. THE GLOBAL BURDEN OF INFECTIOUS AND PARASITIC DISEASES
Despite major progress in microbiological research, infectious and parasitic diseases continue to be a significant burden of disease worldwide. Traditionally, these diseases were described using health data from routine surveillance systems or epidemiological studies. Such data sources are often incomplete or unreliable, and studies that investigate particular conditions are often found to exaggerate claims on mortality. The latter is largely a reflection of comorbidity, in which several coexisting pathologies contribute to and compete for the cause of death.
The Global Burden of Disease (GBD) study of 1990 addressed these problems and quantified the burden of over 100 major disease groups, including infectious diseases, by using a novel and single metric, the disability-adjusted life year (DALY). DALYs express the years of life lost to premature death (YLL) and the years lived with disability (YLD) for varying degrees of severity, making time itself the common metric for death and disability [1]. One DALY is, therefore, a health gap measure, equaling 1 year of healthy life lost. Moreover, DALYs are internally consistent and disaggregate comorbidity, hence decoupling epidemiological measures from advocacy.
The GBD study estimated that, in 1990, over 31% of DALYs worldwide were due to communicable diseases (Table 1) [1, 2]. The vast majority of those occurred in developing countries, where 35% of DALYs were lost to infectious and parasitic diseases, whereas only a little over 4% of the burden in developed regions could be attributed to these disorders. The past 50 years have seen a dramatic decline in the burden of communicable diseases in established market economies, largely as a result of increased income and education and technological advances in sanitation, antimicrobials, and vaccines. It was, therefore, predicted that the burden of infectious diseases may decrease in less developed regions as their incomes rise and access to technological progress improves.
TABLE 1
Global Burden of Disease in 1990 and 2000
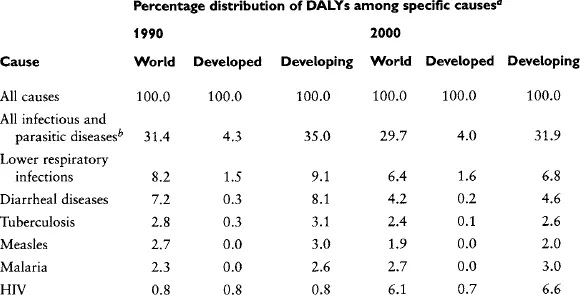
aDALYs, disability-adjusted life years.
bIncludes respiratory infections.
Although progress has been made with respect to some infectious diseases, including respiratory infections, diarrheal diseases, and measles (Table 1), the overall picture has changed little a decade later. Infectious and parasitic diseases still account for nearly 30% of the global burden in the year 2000 (Table 1) and for nearly 32% of the burden in developing countries [2]. Among the top ten leading causes of DALYs worldwide in the year 2000, five were infectious diseases: lower respiratory infections (the number one cause), HIV–AIDS, diarrheal diseases, malaria, and tuberculosis. The situation is particularly bleak in Africa, where 60% of the burden is caused by infectious and parasitic diseases [2]. The surge of the HIV–AIDS epidemic, which is currently causing 6.1% of the total burden and 5.3% of all deaths worldwide, is the major factor responsible for this discouraging score [2]. It largely explains why 26% of all deaths worldwide are still caused by communicable diseases, compared to 27% in 1990.
Whereas the number and rates of death from some communicable diseases, including measles, tuberculosis, and diarrheal diseases, have fallen over the past 10 years, others such as malaria and HIV have increased, particularly in developing countries [2]. This has been accompanied by a worldwide increase in the proportion of DALYs due to noncommunicable diseases from 36% in 1990 to nearly 40% in 2000. Developing countries therefore are experiencing a “double burden” from both communicable and noncommunicable diseases [2]. Given the enormous scope of vaccine technology in combating infectious diseases, efforts to improve access to these resources must therefore remain a major priority in health policy. The analysis of the global burden of infectious disease over the past decade shows that public health interventions against communicable diseases have seen both triumphs and setbacks; it is the purpose of this article to take the reader through past achievements and future opportunities in vaccinology,
II. BRIEF HISTORICAL PERSPECTIVE OF VACCINOLOGY
Vaccination, or the practice of artificially inducing immunity, has been and continues to be one of the most important public health interventions in history, The practice of vaccination can be traced to as early as the seventh century when Indian Buddhists drank snake venom to induce immunity, possibly through a toxoid-like effect [3]. Variolation against smallpox probably began early in the second millenium in central Asia and then spread east to China and west to Turkey [4]. Lady Mary Wortley Montagu introduced variolation into England during 1721 after observing the practice in Constantinople. By using local knowledge regarding the protective effects of cowpox and experimenting further with it, in 1798 Edward Jenner introduced the notion of large-scale, systematic immunization against smallpox by person-to-person inoculation with cowpox virus [4].
The field of vaccinology experienced its next major advance in the 1800s with the concepts of attenuation and virulence. The concept of “passage” of the immunizing agent between animals or humans was recognized as important to maintain its “strength.” In 1885, Louis Pasteur developed the first human vaccine against rabies [5]. In 1886, the concept of killed vaccine was developed when Salmon and Smith produced a killed hog cholera vaccine [6, 7]. This led to three new killed vaccines for humans: against cholera and typhoid in 1896 and against plague in 1897 [4]. Thus, by the end of the nineteenth century, two live attenuated viral vaccines (rabies and smallpox) and three killed bacterial vaccines (typhoid, plague, and cholera) were available for humans.
In the early twentieth century, toxoids were developed against diphtheria and tetanus [8–10], and by 1927, bacille Calmette–Guerin (BCG) vaccine was also available [11]. The isolation of the yellow fever virus in 1927 led to the French strain yellow fever vaccine, followed by the 17D strain, which had fewer side effects [4]. By 1936, two killed influenza vaccines were developed, followed by a live one in 1937. Vaccines against rickettsia ensued, in particular against Q–fever and typhus, the latter in heavy demand during World War II [11]. The first trials for pertussis vaccine, conducted in 1923 and 1924 on the Faroe Islands, led to the availability of several whole cell pertussis vaccines of varying efficacy by the 1940s [12, 13].
The advent of tissue culture in the 1940s sparked the next flurry of vaccine development, allowing for large-scale vaccine production [11]. This new technique made it possible for Enders, Robbins, and Weller to grow poliovirus in tissue culture, winning a Nobel prize for their achievements and leading to the licensure of the Salk and Sabin polio vaccines in 1955 and 1960, respectively [14]. During the 1960s, measles and mumps vaccines were licensed as well as the Japanese encephalitis vaccine, followed by the licensure of rubella and varicella vaccines in the 1970s [4]. The availability of many new vaccines created enormous potential to control several lethal diseases.
III. THE SMALLPOX ERADICATION ERA
Smallpox, one of the deadliest scourges known to humans, was prevalent throughout the world by the seventeenth century. The disease had a profound impact on history, wiping out large populations where it was introduced. It decimated Native American populations and contributed to the demise of the Inca and Aztec empires. In Europe alone, approximately 400,000 persons died annually from smallpox by the end of the eighteenth century [15]. The disease was endemic in populations large enough to sustain transmission, with periodic epidemics every 4–7 years [16]. In smaller or more isolated populations, the disease tended to “burn out,” but would resurge when the virus was reintroduced among enough susceptibles to sustain transmission. By using the cowpox-derived vaccine, smallpox transmission was greatly reduced in Europe after World War ...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- Dedication
- CONTRIBUTORS
- PREFACE
- ACKNOWLEDGMENTS
- Chapter 1: GLOBAL BURDEN OF DISEASE: PART A. The Burden of Vaccine-Preventable Diseases
- Chapter 1: GLOBAL BURDEN OF DISEASE: PART B. Cost Effectiveness of Immunization: Asking the Right Questions
- Chapter 1: GLOBAL BURDEN OF DISEASE: PART C. Potential and Existing Impact of Vaccines on Disease Epidemiology
- Chapter 2: IMMUNOLOGY: PART A. Basic Immunology of Vaccine Development
- Chapter 2: IMMUNOLOGY: PART B. Immunological Requirements for Vaccines To Be Used in Early Life
- Chapter 3: TRIAL DESIGN FOR VACCINES: PART A. Clinical Development of New Vaccines: Phase 1 and 2 Trials
- Chapter 3: TRIAL DESIGN FOR VACCINES: PART B. Phase 3 Studies of Vaccines
- Chapter 4: ETHICS AND VACCINES
- Chapter 5: UNDERSTANDING MICROBIAL PATHOGENESIS AS A BASIS FOR VACCINE DESIGN: PART A. Bacteria
- Chapter 5: UNDERSTANDING MICROBIAL PATHOGENESIS AS A BASIS FOR VACCINE DESIGN: PART B. Disease-Oriented Approach to the Discovery of Novel Vaccines
- Chapter 5: UNDERSTANDING MICROBIAL PATHOGENESIS AS A BASIS FOR VACCINE DESIGN: PART C. Immunological Memory and Vaccines against Acute Cytopathic and Noncytopathic Infections
- Chapter 5: UNDERSTANDING MICROBIAL PATHOGENESIS AS A BASIS FOR VACCINE DESIGN: PART D. Parasitic Diseases, with an Emphasis on Experimental Cutaneous Leishmaniasis
- Chapter 6: DISEASE STATES AND VACCINES: SELECTED CASES: PART A. Introduction
- Chapter 6: DISEASE STATES AND VACCINES: SELECTED CASES: PART B. Polio
- Chapter 6: DISEASE STATES AND VACCINES: SELECTED CASES: PART C. Rubella
- Chapter 6: DISEASE STATES AND VACCINES: SELECTED CASES: PART D. Pertussis
- Chapter 6: DISEASE STATES AND VACCINES: SELECTED CASES: PART E. Rotavirus
- Chapter 6: DISEASE STATES AND VACCINES: SELECTED CASES: PART F. AIDS Vaccines: Challenges and Prospects
- Chapter 6: DISEASE STATES AND VACCINES: SELECTED CASES: PART G. Pneumococcus, Pneumococcal Disease, and Prevention
- Chapter 6: DISEASE STATES AND VACCINES: SELECTED CASES: PART H. Tuberculosis
- Chapter 6: DISEASE STATES AND VACCINES: SELECTED CASES: PART I. Malaria
- Chapter 6: DISEASE STATES AND VACCINES: SELECTED CASES: PART J. Human Papillomaviruses
- Chapter 6: DISEASE STATES AND VACCINES: SELECTED CASES: PART K. Helicobacter Pylori
- Chapter 6: DISEASE STATES AND VACCINES: SELECTED CASES: PART L. Genome-Based Approach for a Vaccine against Neisseria meningitidis
- Chapter 7: ECONOMICS OF VACCINES: FROM VACCINE CANDIDATE TO COMMERCIALIZED PRODUCT
- Chapter 8: VACCINE SAFETY: REAL AND PERCEIVED ISSUES
- Chapter 9: INTRODUCTION OF NEW VACCINES IN THE HEALTHCARE SYSTEM
- Chapter 10: FUTURE CHALLENGES FOR VACCINES AND IMMUNIZATION
- INDEX
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access The Vaccine Book by Barry R. Bloom,Barry R. Bloom,Paul-Henri Lambert in PDF and/or ePUB format, as well as other popular books in Medicine & Epidemiology. We have over 1.5 million books available in our catalogue for you to explore.