- 420 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Liver Disorders in Childhood provides a comprehensive account of disorders of the liver and biliary system in childhood. Topics covered include the mechanisms of physiological jaundice; the link between jaundice and breast feeding; surgery for extrahepatic biliary atresia; the role of hepatitis B virus infection in chronic liver disease; presymptomatic diagnosis of Wilson's disease; liver transplantation; and surgical treatment of metabolic disorders such as glycogen storage disease. The main focus is on day-to-day practical problems of diagnosis and management from the viewpoint of the pediatrician. This book consists of 22 chapters and begins with an overview of the anatomy and physiology of the liver and the biliary tract. The discussion then turns to liver disorders such as conjugated and unconjugated hyperbilirubinemia; extrahepatic biliary atresia; infections of the liver; fulminant hepatic failure; and Reye's syndrome (encephalopathy and fatty degeneration of the viscera). Liver disorders caused by drugs or toxins are also considered, along with inborn errors of metabolism causing hepatomegaly or disordered liver function; familial and genetic structural abnormalities of the liver and biliary system; chronic hepatitis; and Wilson's disease. This monograph is written primarily for clinicians, especially pediatricians, paediatric surgeons and gastroenterologists, but will also be of value to pathologists, biochemists, and laboratory research workers concerned with understanding aspects of hepatic function and elucidating pathogenic mechanisms.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineCHAPTER 1
Anatomy and Physiology of the Liver
Publisher Summary
The liver is essentially a mass of cells permeated by a complex but ordered system of channels carrying its blood supply and bile. Electron microscopic examination of hepatocytes shows an equally complex arrangement of channels connecting intracellular organelles. This chapter explains the structural arrangements which ensure that each hepatocyte is in intimate contact with the blood flowing through the liver, facilitating transport of materials into and out of the hepatocyte, and at the same time facilitating secretion of bile. The liver is a continuous, uniform organ adopting a shape enforced on it by body cavities, other intraperitoneal structures, and vascular forces—the positive pressure from the portal vein and the hepatic artery and the often negative pressure in the hepatic veins. The conventional division into right and left lobes does not coincide with the intrahepatic branching of vessels and ducts. Some knowledge of the normal distribution of these structures is necessary to understand some of the pathological consequences of disease within the liver or in the portal venous system.
Clinical assessment of liver
Inspection
Where hepatomegaly is massive, or where there are large nodules on the surface of the liver, this may be evident on inspection.
Palpation and percussion
The lower edge of the liver should be palpated just lateral to the right rectus muscle. In the newborn and in the first four months of life, the liver edge may be palpable up to 2 cm below the costal margin without indicating hepatomegaly. In older children, it is rarely more than 1cm below the costal margin, except in deep inspiration. It may be normally palpable in the mid-line 3 or 4 cm below the base of the xiphisternum.
If the liver is palpable at a lower level, one cannot immediately conclude that the liver is enlarged until the position of the upper border has been determined by percussion. It should be at the level of the fifth or sixth rib in the right mid-axillary line, at about the seventh intercostal space in the mid-axillary line, and at the ninth rib posteriorly. There is some doubt as to whether light percussion is more informative than heavy percussion for this purpose. I favour the former, but it is probably more important for a clinician to use a consistent method and interpret the results with some allowance for the effect of subcutaneous fat, oedema, and the state of the lungs. Emphysema displaces downwards the upper limits of hepatic dullness. The left lobe extends from the mid-line out as far as the left mid-clavicular line.
A Reidel’s lobe is a downward tongue-like projection from the right lobe of the liver. It may extend as far as the right iliac crest.
Percussion is of value in detecting a reduction in the size of the liver. In cirrhosis the area of hepatic dullness will have a lower upper border than normal and dullness will stop well above the edge of the rib cage.
Very large livers are associated with storage disorders, disorders of the reticulo-endothelial system, such as leukaemia, gross fatty change, malignant disease and congestive cardiac failure. Rapid changes in size occur in congestive cardiac failure and in bile duct obstruction.
Some information on the nature of the liver disease may be inferred from the consistency of the edge of the liver and from its surface. The normal edge is soft, fairly sharp, and is not tender. Livers swollen because of congestive cardiac failure, or acute hepatocyte infiltration are firm, have somewhat rounded edges, smooth surfaces and are tender if the swelling is acute. In cirrhosis the liver is hard and has an irregular surface and edge. The liver is pulsatile in tricuspid incompetence.
Auscultation
Auscultation is of value in detecting increased hepatic blood flow in vascular lesions such as tumours and haemangiomata. It has also been used to try to assess the position of the lower border of the liver. A stethescope may be placed on the xiphisternum and the abdomen scratched lightly in a transverse direction, advancing the line of the scratch cephalad in the right mid-clavicular line. If the edge of the liver is below the costal margin a change in intensity and quality of the auscultated sound is noted as the edge is crossed. In general, this technique has little to add to palpation, but it may be helpful when the liver is large but soft; for example, in glycogen storage disease.
Where serial recordings of liver size are desirable, the most consistent is that obtained by palpating the edge of the liver in the right mid-clavicular line recording the distance below the rib cage at which the edge is palpable. An alternative method is to determine the upper limit of hepatic dullness in the mid-clavicular line and to record the distance between this point and the palpated edge of the liver in the mid-clavicular line. Where the latter technique has been compared with isotope scintiscans, considerable discrepancies have been found.
Spleen
The spleen can be palpated from 1 to 2 cm below the left costal margin during the first few weeks of life. The tip is often palpable in well infants and young children. It is very commonly enlarged during generalized infections. Gentle palpation starting from the right iliac fossa and moving towards the left costal margin is the best technique. The spleen is a very superficial organ, and the edge is very distinct. The splenic notch is very rarely palpable. On percussion the dullness extends up beyond the costal margin. Careful palpation and percussion detects the vast majority of spleens which have been shown to be enlarged by scintiscanning. The scintiscan is particularly valuable in the presence of ascites.
ANATOMY OF THE LIVER
The liver is essentially a mass of cells permeated by a complex but ordered system of channels carrying its blood supply and bile. Electronmicroscopic examination of hepatocytes shows an equally complex arrangement of channels connecting intracellular organelles. In this chapter emphasis will be given to the structural arrangements which ensure that each hepatocyte is in intimate contact with the blood flowing through the liver, facilitating transport of materials into and out of the hepatocyte, and at the same time facilitating secretion of bile.
Gross structure
The liver is a continuous, uniform organ adopting a shape enforced on it by body cavities, other intraperitoneal structures and vascular forces; the positive pressure from the portal vein and the hepatic artery and the often negative pressure in the hepatic veins. The conventional division into right and left lobes does not coincide with the intrahepatic branching of vessels and ducts. Some knowledge of the normal distribution of these structures is necessary to understand some of the pathological consequences of disease within the liver or in the portal venous system.
Portal vein branches
Since the hepatic artery and bile ducts follow the portal vein and its branches these will be described. The portal vein, which is formed by the junction of the superior mesenteric vein and the splenic vein, is directed towards the right lobe as it approaches the portahepatis. It branches into a short right trunk and a longer left trunk. The intrahepatic branches are subject to minor variations but a ‘typical’ pattern can be described. The right branch gives rise to a lateral branch directed to the right upper lobe, an inferior branch supplying the area to the right of the gallbladder and a large central branch supplying the antero-superior portion of the liver. From the left trunk, superior, intermediate and inferior branches supply the lateral aspects of the left lobe and branches run also to the caudate and quadrate lobes (Figure 1.1). Anastomoses between the branches of the right and left portal vein branches are unusual. Each terminal branch has a sharply defined territory, the smaller branches having the characteristic of ‘end-arteries’. The portal vein ‘territories’ are shared by branches of the hepatic artery and tributaries of the hepatic duct which accompany the veins.
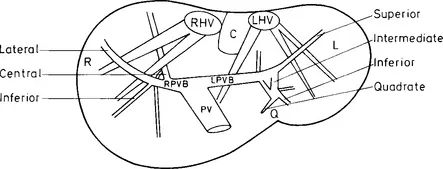
Figure 1.1 Diagrammatic representation of portal blood distribution to the right (R), left (L), quadrate (Q), and caudate (C) lobes of the liver, and the main right (RHV) and left (LHV) hepatic veins
Hepatic artery
The hepatic artery and its intrahepatic branches are much less constant. In 55 per cent of individuals the main hepatic artery arises as a single trunk from the coeliac artery but in the remainder two or three main arteries arise from the coeliac, superior mesenteric, gastro-duodenal, left or right gastric arteries, or even direct from the aorta.
Within the liver the artery or its branches follow the appropriate branches of the portal vein. Sometimes two anastomosing arteries may accompany one vein, but the terminal branches are end-arteries supplying independently a circumscribed volume of liver. There are no intrahepatic communications between the right and left hepatic arteries.
Hepatic vein tributaries
The hepatic vein tributaries have sharply defined areas of drainage which do not relate directly to the portal vein end-branch or hepatic end-artery territory, yet they do interdigitate with these to give uniform drainage of the liver. On both a microscopic and a macroscopic scale, portal vein and hepatic veins run as nearly perpendicular to one another as is geometrically possible. There are three main hepatic veins: the right hepatic vein drains the right upper lobe, the middle vein drains an area supplied by both the right ...
Table of contents
- Cover image
- Title page
- Table of Contents
- POSTGRADUATE PAEDIATRICS SERIES
- Copyright
- Dedication
- Editor’s Foreword
- Preface
- Chapter 1: Anatomy and Physiology of the Liver
- Chapter 2: Anatomy and Physiology of the Biliary Tract
- Chapter 3: Unconjugated Hyperbilirubinaemia
- Chapter 4: Conjugated Hyperbilirubinaemia
- Chapter 5: Extrahepatic Biliary Atresia
- Chapter 6: Infections of the Liver
- Chapter 7: Fulminant Hepatic Failure
- Chapter 8: Reye’s Syndrome: (Encephalopathy and fatty degeneration of the viscera)
- Chapter 9: Liver Disorders Caused by Drugs or Toxins
- Chapter 10: Inborn Errors of Metabolism Causing Hepatomegaly or Disordered Liver Function
- Chapter 11: Familial and Genetic Structural Abnormalities of the Liver and Biliary System
- Chapter 12: Chronic Hepatitis
- Chapter 13: Wilson’s Disease
- Chapter 14: Cirrhosis and its Complications
- Chapter 15: Hepato-biliary Lesions in Cystic Fibrosis
- Chapter 16: Liver and Gallbladder Disease in Sickle Cell Anaemia
- Chapter 17: Indian Childhood Cirrhosis
- Chapter 18: Disorders of the Portal and Hepatic Venous Systems
- Chapter 19: Liver Tumours
- Chapter 20: Disorders of the Gallbladder and Biliary Tract
- Chapter 21: Laboratory Assessment of Hepatobiliary Disease
- Chapter 22: Investigation of Biliary Tract Disease
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Liver Disorders in Childhood by Alex P. Mowat, John Apley in PDF and/or ePUB format, as well as other popular books in Medicine & Gynecology, Obstetrics & Midwifery. We have over 1.5 million books available in our catalogue for you to explore.