- 317 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Lasers and Optical Fibers in Medicine
About this book
The increasing use of fiber optics in the field of medicine has created a need for an interdisciplinary perspective of the technology and methods for physicians as well as engineers and biophysicists. This book presents a comprehensive examination of lasers and optical fibers in an hierarchical, three-tier system. Each chapter is divided into three basic sections: the Fundamentals section provides an overview of basic concepts and background; the Principles section offers an in-depth engineering approach; and the Advances section features specific information on systems and biophysical parameters. All those interested in the fields of lasers and fiber optics will find this book fascinating and instructive reading.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
1
Introduction
1.1 HISTORICAL BACKGROUND
Light has been used by physicians for both diagnostic and therapeutic procedures since the dawn of civilization. Observation being the only diagnostic tool, light enabled them to see skin color, inspect eyes or wounds, and then choose a suitable course of therapy. Heat from sunlight, or even from light emitted from campfires, was used for therapy throughout the ages. Both the Greeks and the Romans used to take daily sunbaths and a solarium was part of many Roman houses. Illumination by sunlight was used in ancient Egypt for therapeutic application in skin diseases.
Even during the early days of medicine it was clearly understood by physicians that they would benefit enormously if they could diagnose and treat the inside of the body using nonsurgical medical instruments. One of the first attempts was the development of a simple optical instrument to look inside the body. A tube inserted into the ear or the mouth enabled some limited view inside the body and was called an endoscope. The word endoscope stems from the Greek endo—within, and skopien—to view. Over the last few hundred years these instruments have been much improved mechanically and optically. With the availability of optical fibers and lasers, the endoscope became a more complicated but much more powerful diagnostic as well as therapeutic tool. The new fiberoptic endoscopes and “integrated” systems such as the laser catheter or the laser endoscope were to cause a revolution in many fields of medicine. If one can position optical fibers at a desired spot in the body, these systems cover virtually all the medical procedures, such as diagnosis, surgery, and therapy, with greatly reduced trauma to the patient. This book deals with this rapid expansion of laser and fiberoptic technology in medicine.
By way of introduction, the various stages that led to the development of the modern endoscopic systems are discussed (Berci, 1976; Haubrich, 1987). The first phase of endoscopy is based on hollow tubes and rudimentary optical elements. Many centuries before Christ, simple open tubes were used for the examination of body cavities. It was only in the early 1800s that Bozzini added improved illumination by using a wax candle light source and a 45° mirror to reflect light into the tube. Desormeaux made further improvements in 1867 by replacing the candle with an alcohol flame and the mirror with a lens. This type of rigid endoscope was inserted for the first time in 1868 by Kussmaul through the mouth, pharynx and esophagus, making it possible for the inside of the stomach to be seen. It is said that a professional sword swallower volunteered to be the first patient. This was a first attempt at gastroscopy. A few of the very early endoscopes are shown in Fig. 1.1.
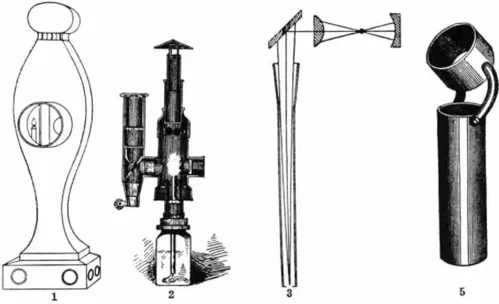
FIGURE 1.1 Earliest endoscopes: (1) Bozzini’s apparatus; (2) Desormeaux’s illuminating apparatus; (3 and 5) Kussmaul’s and Bevan’s esophagoscopes. (Courtesy of the Medical Library of the University of Vienna.)
Later in the 1800s there were further developments, such as the construction of several tubes which were telescoped into each other to facilitate easier introduction into the body. An element of flexibility was added by building part of the instrument with metal rings rather than from a rigid tube. In this first stage of endoscopy, the organ inside the body was illuminated through the tube and the physician looked directly at the organ through the tube. Another stage in the development of endoscopes was the use of a simple optical system for transmission of a full image from inside the body to the physician’s eyes. One of the pioneers of this was Nitze, who in 1879, in collaboration with the instrument maker Leiter and others, placed a lens into an open tube and used a glowing platinum wire as a light source. He later used a miniature electric globe for this purpose (Lewandowski, 1892). At the same time Edison was making his improved electric bulbs, which were used by Mikulicz in 1881 to build better gastroscopes. Similar instruments were being made for use in other areas of medicine, such as the bronchoscope or cystoscope, and were gradually improved throughout the early 1900s. One of the improvements included a rubber tube, which was introduced first and served as a guide for the rigid endoscope. Another was an endoscope whose distal end was movable. It should be noted that as early as 1890, these endoscopists were using still cameras to record their findings. Musehold, for example, had photographed the larynx in 1893. A few of the endoscopes of this period are shown in Figs. 1.2–1.4.
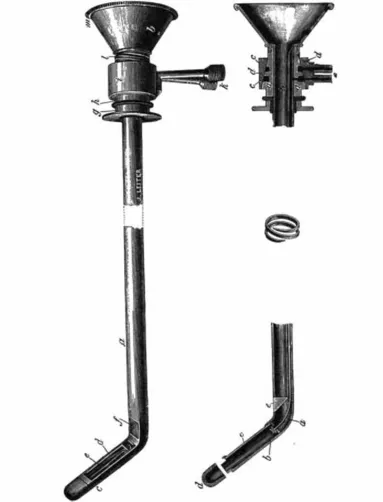
FIGURE 1.2 Leiter rigid endoscopes with bent tip. (From Lewandowski, 1892. Courtesy of the Medical Library of the University of Vienna.)

FIGURE 1.3 A porter carrying the Nitze-Leiter cytoscope (1879). (Courtesy of the Medical Library of the University of Vienna.)
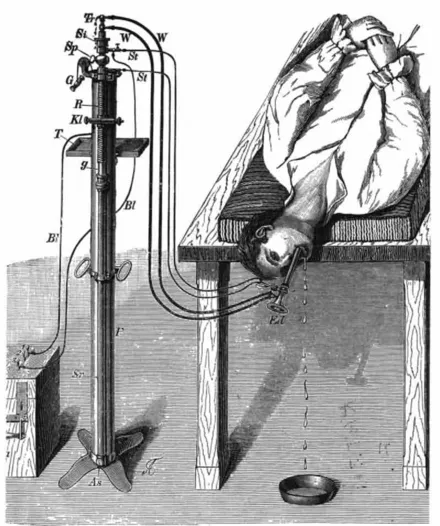
FIGURE 1.4 Mikulicz gastroscope. (From Lewandowski, 1892. Courtesy of the Medical Library of the University of Vienna.)
The second phase in the development of endoscopes was the use of a series of lenses, rather than a single element, to transmit images. An important development was made by Schindler and Wolf in Germany in 1936, when they built a semiflexible gastroscope, consisting of a series of lenses. A further advancement was implemented by H. H. Hopkins in the 1940s in Britain by using a novel rod-lens system which produced a better-quality image. Hopkins-type endoscopes are still widely used today, as shown in Fig. 1.5. 1 During the first half of the 20th century, the rapid development of photographic technology was incorporated into endoscopy. First, color photographs were taken during gastroscopy, and later motion pictures were taken of the larynx, the esophagus, and the bronchial tree.
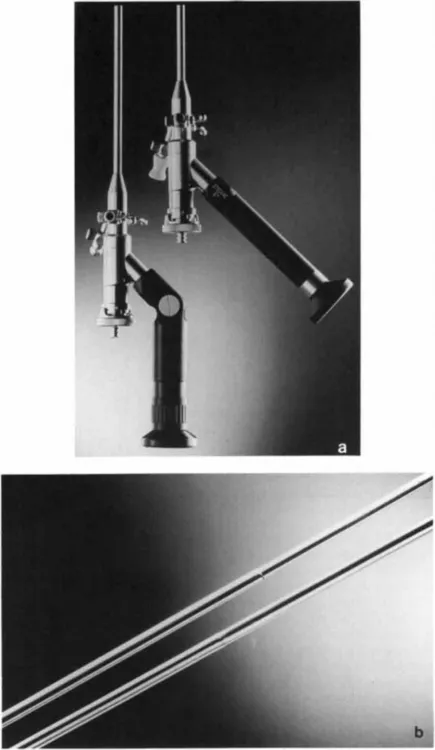
FIGURE 1.5 Modern (Hopkins-type) rigid endoscopes: (a) proximal and (b) distal ends. (Courtesy of Storz.)
The third phase in the development of endoscopy was the introduction of fiberoptic endoscopes. These are based on thin and transparent threads of glass, the so-called optical fibers. The idea of transmitting images by using bundles of optical fibers dates back to the years 1927–1930 and to the independent work of J. L. Baird in the United Kingdom, C. W. Hansell in the United States, and H. Lamm in Germany. The idea lay dormant for two decades until it was revived independently in 1954 by A. C. S. van Heel in Holland and by H. H. Hopkins and N. S. Kapany in England. These researchers demonstrated that a bundle of thin optical fibers could be used to transmit a good-quality image, and with the improved flexibility of the fiber bundle the potential applications for optical fibers in medicine could be greatly expanded. In 1959 the first medical instrument, a flexible fiberoptic gastroscope (Hirschowitz, 1979), was developed and used on patients by a physician (Hirshowitz) working in conjunction with two physicists (Curtiss and Peters). An early endoscope and an image transmitted through it are shown in Fig. 1.6 and Fig. 1.7.
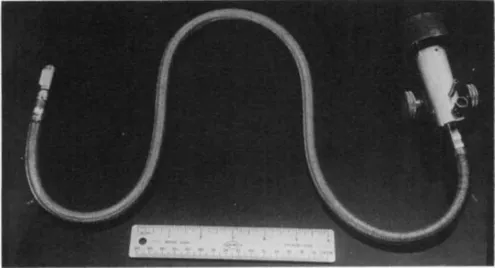
FIGURE 1.6 An early fiberoptic endscope. (Courtesy of B.I. Hirschowitz.)
FIGURE 1.7 Photograph of a stamp taken through the endoscope pictured in Fig. 1.6. (Courtesy of B. I. Hirschowitz.)
Soon afterward, other fiberoptic endoscopes followed, such as bronchoscopes and colonoscopes. In these flexible endoscopes, the fiberoptic system provided both the illumination and the image transmission. Most of the endoscopes incorporated open (ancillary) channels through which the physician could inject saline solution or drugs or insert instruments such as forceps or electrosurgical instruments. An early commercial endoscope and a picture taken through it are shown in Fig. 1.8 and Fig. 1.9.

FIGURE 1.8 Early commercial fiberoptic gastroscope. (Courtesy of Olympus.)
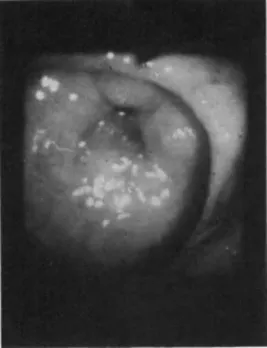
FIGURE 1.9 Picture of a stomach taken through the endoscope pictured in Fig. 1.8. (Courtesy of Olympus.)
In the early 1970s, there was rapid development in the field of optical fibers for communications. Optical fibers of superb quality and excellent transmission were produced for application in communication networks. Applied to endoscopy, these fibers brought about huge improvements; for example, thin endoscopes were developed for cardiology (angioscopes). These endoscopes have an outer diameter of less than 3 mm and incorporate more than 10,000 individual fibers in their imaging bundle to greatly enhance the optical resolution. They also include an ancillary channel for irrigation or for insertion of an additional instrument. These thin instruments enable physicians to obtain images from areas which were, until now, quite beyond their reach.
In 1960, the first laser (the ruby laser) was developed by T. Maiman. This new source of light has many technological and military applications. Ever since the first laser was developed, it was believed that lasers would have a far-reaching impact on medicine. In particular, three properties were recognized as extremely important: (a) the laser emits a collimated (parallel) beam of light, which can be very powerful; (b) the light is practically monochromatic (consisting of one color); and (c) one of the unique features of laser light, known as coherence, makes it possible to focus it onto a very small spot. The energy density (energy divided by irradiated area) in this focal spot is high, and when the light is absorbed in biological tissue it can cause a rapid rise in temperature. At low energy levels, the heat generated in the spot coagulates blood and causes hemostasis (bleeding ceases) of small blood vessels. At higher levels, it causes vaporization and removal of tissue. These are the basic phenomena used in laser surgery. During the four years following the invention of the first laser, three other lasers were invented: the Ar (argon) ion, the CO2 (carbon dioxide), and the Nd:YAG (neodymium : yttrium aluminum g...
Table of contents
- Cover image
- Title page
- Table of Contents
- Physical Techniques in Biology and Medicine
- Copyright
- Dedication
- Preface
- Prologue
- Chapter 1: Introduction
- Chapter 2: Medical Lasers
- Chapter 3: Applications of Lasers in Therapy and Diagnosis
- Chapter 4: Single Optical Fibers
- Chapter 5: Optical Fiber Bundles
- Chapter 6: Endoscopy
- Chapter 7: Fiberoptic Diagnosis
- Chapter 8: Fiberoptic Laser Systems for Diagnostics and Therapy
- Chapter 9: Clinical Applications of Fiberoptic Laser Systems
- Appendix
- Glossary
- Bibliography
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Lasers and Optical Fibers in Medicine by Abraham Katzir in PDF and/or ePUB format, as well as other popular books in Biological Sciences & Biophysics. We have over 1.5 million books available in our catalogue for you to explore.