- 296 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Medical Microbiology Illustrated
About this book
Medical Microbiology Illustrated presents a detailed description of epidemiology, and the biology of micro-organisms. It discusses the pathogenicity and virulence of microbial agents. It addresses the intrinsic susceptibility or immunity to antimicrobial agents. Some of the topics covered in the book are the types of gram-positive cocci; diverse group of aerobic gram-positive bacilli; classification and clinical importance of erysipelothrix rhusiopathiae; pathogenesis of mycobacterial infection; classification of parasitic infections which manifest with fever; collection of blood for culture and control of substances hazardous to health. The classification and clinical importance of neisseriaceae is fully covered. The definition and pathogenicity of haemophilus are discussed in detail. The text describes in depth the classification and clinical importance of spiral bacteria. The isolation and identification of fungi are completely presented. A chapter is devoted to the laboratory and serological diagnosis of systemic fungal infections. The book can provide useful information to microbiologists, physicians, laboratory scientists, students, and researchers.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
1
Introduction to clinical microbiology
Publisher Summary
This chapter discusses the process of microbiological diagnosis from the initial clinical encounter to the completion of the diagnostic and therapeutic process. The process of making a microbiological diagnosis has many component steps. The process begins when the clinician meets the patient, takes a history, and performs a clinical examination. The clinician forms a hypothesis about the cause of the patient’s complaint: the differential diagnosis. With this hypothesis, a diagnostic is constructed that will include laboratory, radiological, and other investigations. Relevant specimens are obtained and transported to the laboratory. It is essential that this process is closely controlled as most microbiological specimens are highly perishable. When they are received in the laboratory, the specimens should be carefully documented and urgent specimens identified for rapid processing. They should then be investigated according to the standard laboratory procedures. A report is drawn up that may indicate the presence or absence of human pathogens and, where relevant, their susceptibility to anti-microbial agents. These results are communicated to the clinician together with further advice from the clinical microbiologist, who may request further specimens, modifications to the treatment regimen, or clinical and laboratory follow-up.
Introduction
A detailed understanding of epidemiology, and the biology of micro-organisms is required if patients with infectious diseases are to be adequately treated. Knowledge of the normal resident microbial flora facilitates the evaluation of the significance of individual organisms isolated from clinical specimens. An understanding of the pathogenicity and virulence will assist in predicting the likely behaviour of potential pathogens. In the same way, knowledge of intrinsic susceptibility or resistance to antimicrobial agents will be valuable in planning effective antimicrobial chemotherapy. This introductory chapter discusses the process of microbiological diagnosis from the initial clinical encounter to the completion of the diagnostic and therapeutic process.
The process of microbiological diagnosis
The process of making a microbiological diagnosis has many component steps. All of these must be understood and optimized if the laboratory is to collaborate fully with the clinician in achieving the best outcome for the patient.
The process begins when the clinician meets the patient, takes a history and performs a clinical examination. The clinician forms a hypothesis about the cause of the patient’s complaint: the differential diagnosis. With this hypothesis a diagnostic plan must be constructed which will include laboratory, radiological and other investigations. At this point the clinical microbiologist may be contacted and discussions may lead to the development of the differential diagnosis. The clinical microbiologist can also advise on the most appropriate investigations, how the specimens should be sent and may also give advice on empirical therapy.
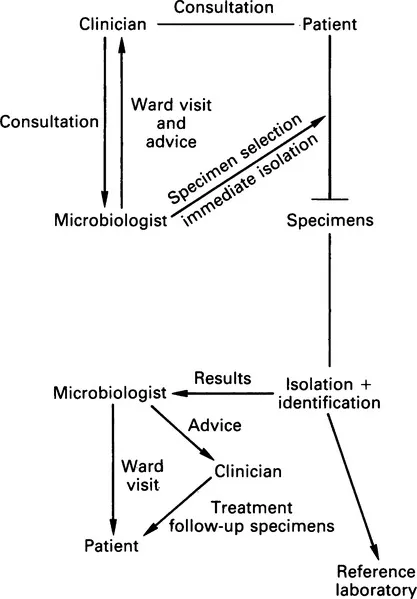
Relevant specimens are obtained and transported to the laboratory. It is essential that this process is closely controlled as most microbiological specimens are highly perishable. When they are received in the laboratory the specimens should be carefully documented and urgent specimens identified for rapid processing. They should then be investigated according to the standard laboratory procedures. A report is drawn up which may indicate the presence or absence of human pathogens and, where relevant, their susceptibility to antimicrobial agents. These results are communicated to the clinician, together with further advice from the clinical microbiologist, who may request further specimens, modifications to the treatment regimen or clinical and laboratory follow up. This is summarized in Figure 1.1.
Specimens
The quality of microbiological specimens is crucial to the value of the results obtained. For example the possibility of isolating an organism is much reduced if antibiotics are given before a specimen is obtained.
Specimen types
Specimens may be divided into two groups: those from normally sterile sites, and those containing normal bacterial flora. It is important to classify them in this way as it affects the way in which they are processed, culture results are evaluated and reports issued.
Specimens from sites which are normally sterile are inoculated into enrichment media. This protects fastidious pathogens that may be present in small numbers, provides all essential nutrients, and allows rapid multiplication so that enough organisms will be available for identification and susceptibility testing. By contrast, in specimens from a site with a normal flora, selective agents must be used to suppress the growth of commensal organisms which would obscure any pathogens. Thus for specimens from sterile sites amplification is the aim whereas for sites with a normal flora selection is the aim.
The isolation of an organism from a site which is normally sterile is likely to be clinically important. Organisms may be present as a result of contamination during the clinical procedure required to collect it or during laboratory processing. Before an organism is dismissed as a contaminant, careful evaluation must be made of the clinical details usually by a visit to the patient.
In many instances, the interpretation of bacterial isolates is made more complex when important pathogenic organisms form part of the normal flora in asymptomatic subjects. Streptococcus pneumoniae may be found in the nasopharynx of up to 30% of healthy adults. Sputum specimens are contaminated with pharyngeal secretions which may therefore contain this organism. To overcome this problem quantitative techniques have been evolved which assume that potential pathogens are present in smaller numbers when they are acting as commensals than when they are acting as pathogens (see p. 181).
Specimen choice
Advice must be given to clinical colleagues on the most appropriate specimens for the investigation of each infective condition: for example in gonorrhoea in females an endocervical swab should be sent rather than a high vaginal swab as the former has a much higher diagnostic yield.
In the investigation of acute lower respiratory tract infection where the patient is unable to produce a satisfactory sputum specimen, more invasive techniques such as broncho-alveolar lavage may be necessary. When an abscess is drained surgically, specimens of pus should be sent in a sterile container or a sterile syringe rather than on a bacteriological swab. Pathological material may dry rapidly causing fastidious organisms to die. Swabs maximize the exposure of bacteria to drying and atmospheric oxygen resulting in a reduction in diagnostic yield; some organisms are inhibited by materials in the swab itself.
Containers
Labelled, sterile containers should be available for collection of microbiological specimens.
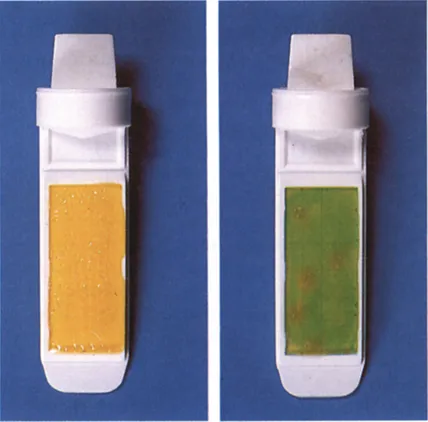
These should be of different sizes, depending on the specimen (i.e. a screw-capped container for cerebrospinal fluid (CSF), a wide-mouth container for mid-stream specimens of urine (MSU)). Stool pots may have a scoop incorporated in the lid to make specimen collection more aesthetic. Bottles should have a label which prompt the clinician to record essential information (i.e. name, hospital number, sex, date of birth) so that they can be reliably identified. Sodium borate can be added to urine containers to inhibit bacterial multiplication. A ‘dip slide container’ may be provided in which there is a paddle coated on both sides with an agar medium (usually MacConkey and cysteine lactose electrolyte deficient (CLED) agars). The paddle is dipped in the urine which is then discarded and the paddle replaced in the container. Organisms survive well on these media at ambient temperature while in transit to the laboratory where they are subsequently incubated at 37°C. Colony counts will be available on the following day and identification and susceptibility tests can be performed by subculture (Fig. 1.2).
Some perishable specimens are collected directly into a transport or culture medium and these require careful stock control to ensure that these media are kept in an optimum condition. Some workers consider that blood cultures collected into blood culture medium which is held at 37°C produces a higher diagnostic yield as this is thought to prevent ‘cold shock’ which retards growth. If this strategy is adopted, the microbiologist must provide blood culture bottles ...
Table of contents
- Cover image
- Title page
- Table of Contents
- Dedication
- Copyright
- Preface
- Acknowledgements
- Chapter 1: Introduction to clinical microbiology
- Chapter 2: Gram-positive cocci
- Chapter 3: Gram-positive bacilli
- Chapter 4: Mycobacterial infection
- Chapter 5: Gram-negative cocci (the Neisseriaceae)
- Chapter 6: Gram-negative coccobacilli
- Chapter 7: Gram-negative bacilli
- Chapter 8: Anaerobes
- Chapter 9: Spiral bacteria
- Chapter 10: Medical mycology
- Chapter 11: Parasitology
- Chapter 12: The microbiology laboratory: organization and quality assurance
- Chapter 13: Safety in the laboratory
- Chapter 14: Collection of blood for culture
- Chapter 15: Examination of specimens from the central nervous system
- Chapter 16: Infections of the respiratory tract
- Chapter 17: Examination of faeces for bacterial pathogens
- Chapter 18: Examination of urine and pus
- Chapter 19: Investigation of specimens from the genital tract and diagnosis of sexually transmitted diseases (STDs)
- Chapter 20: Antimicrobial susceptibility
- Chapter 21: Serological techniques
- Chapter 22: Bacteriological examination of water, food and air
- Further reading
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Medical Microbiology Illustrated by S. H. Gillespie in PDF and/or ePUB format, as well as other popular books in Biological Sciences & Diseases & Allergies. We have over 1.5 million books available in our catalogue for you to explore.