Perinatal cardiology is an important developing field as high quality ultrasound is used on a growing number of pregnant women, and diagnosis prior to birth will become a more common occurrence. In addition, highly sensitive noninvasive diagnostic tools, advances in neonatal care and anesthesia, evolution of transcatheter interventional procedures and performance of complicated surgical procedures in the neonate and young infant have advanced to such an extent that almost all congenital cardiac defects can be diagnosed and "corrected." Illustrated with over 500 figures, this book by leaders in the fields of pediatric cardiology, neonatology, pediatric cardiovascular surgery and interventional pediatric cardiology focuses on congenital heart defect issues during the perinatal period: prenatal (before birth) and neonatal (first month after birth). This book discusses the three major areas of perinatal cardiology: 1. Provides an overview of advances in perinatology, neonatology, cardiology and cardiac surgery in making early diagnosis and offering treatment options for patients with CHD.2. The concept of the multidisciplinary approach to managing infants with congenital cardiac lesion.3. Evidence-based therapeutic approaches to successfully treat the fetus and the newborn with congenital cardiac lesions.
eBook - ePub
Perinatal Cardiology: A Multidisciplinary Approach
A Multidisciplinary Approach
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Perinatal Cardiology: A Multidisciplinary Approach
A Multidisciplinary Approach
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
CardiologySECTION V
Diagnosis and Management
Chapter 10
AN APPROACH TO THE DIAGNOSIS OF CYANOTIC NEONATE FOR THE PRIMARY CARE PROVIDER
Introduction
Newborn infants with distress caused by heart defects may not live unless they are treated correctly and quickly.1–4 Cyanosis is a crucial manifestation of congenital heart defects (CHDs) in the neonate. Pediatric cardiology consultation and/or an echocardiographic study may assist in making a diagnosis. However, such services may not be readily accessible to all newborn babies. An appreciation of the problems related to cyanotic infants by the primary care physician, whether he/she is a pediatrician or a neonatologist, may be useful. At the outset, it should be emphasized that (1) complex physiological and anatomical alterations take place during and immediately after birth5–7; (2) severe cyanotic CHD can exist without a cardiac murmur; (3) a loud murmur does not automatically suggest that the reason for the distress in the baby is related to a heart defect; (4) when a murmur is detected, it is not necessarily characteristic for a specified CHD; and (5) lack of cardiomegaly on a chest x-ray image does not eliminate severe CHD.
In this chapter, the author will name the causes of cyanosis in the newborn infant; delineate techniques to distinguish cardiac from noncardiac causes of cyanosis; and describe an approach to formulate a cardiac diagnosis prior to echocardiographic and Doppler studies.
Causes of Neonatal Cyanosis
The etiology of cyanosis may chiefly be categorized into respiratory, cardiac and central nervous system (CNS) disorders, persistent pulmonary hypertension (PPHN), and a miscellaneous group of abnormalities and are listed in Table 10.1.
Table 10.1. Causes of cyanosis
|
The respiratory disorders may be subgrouped as pulmonary parenchymal disorders and diseases causing mechanical interference with lung function, and are shown in Table 10.2.
Table 10.2. Respiratory disorders causing cyanosis
| A. Pulmonary parenchymal diseases
B. Diseases causing mechanical interference with lung function
|
The cyanotic CHD may be subdivided into 3 groups, depending upon pulmonary vascular markings on a chest x-ray (Table 10.3). PPHN (also referred to as persistent fetal circulation [PFC]) is an important cause of cyanosis; this is because of associated right-to-left shunt across the patent foramen ovale (PFO) and/or patent ductus arteriosus (PDA).
Table 10.3. Heart defects causing cyanosis
| A. Decreased pulmonary vascular markings
B. Increased pulmonary vascular markings
C. Severe pulmonary venous congestion
|
CNS disorders, which are likely to cause cyanosis, are shown in Table 10.4; the cyanosis as a rule is related on hypoventilation.
Table 10.4. CNS disorders causing cyanosis
|
A remarkable group of miscellaneous disorders, which may cause cyanosis, are listed in Table 10.5.
Table 10.5. Miscellaneous disorders causing cyanosis
|
Cardiac versus Noncardiac
A diagnosis of the cause of the cyanosis (see Tables 10.1–10.5) can frequently be accomplished by the use of usual clinical evaluation and laboratory studies. Respiratory causes may be assumed if there were complications during pregnancy and/or delivery, fever in the mother before birth, onset of cyanosis within the first few hours following birth, prematurity, inappropriate weight for gestational age, asphyxia neonatorum, meconium staining, and/or low Apgar score. Chest x-ray will more often than not aid in recognizing respiratory problems caused by lung parenchymal disease and those that produce mechanical interference with lung function (see Table 10.2). Arterial blood gas examination is helpful in distinguishing cardiac from lung diseases. The PaCO2 is increased in pulmonary disorders, but not consistently so in CHDs. Nevertheless, there are some babies in whom it is not easy to distinguish between severe pulmonary disease (PD) and cyanotic CHD.
Improvement in arterial PO2 following 100% oxygen administration in an oxyhood for a period of 15 minutes1,9 is helpful in the differential diagnosis; significant increase in the PO2 occurs in infants with PD while no noteworthy increase in PO2 (< 10 torr) is seen in cyanotic CHD babies. A PaO2 >150 torr is extremely suggestive of pulmonary problem. A higher PO2 in the right radial artery blood sample than that in the umbilical artery sample is suggestive of right-to-left shunt via the ductus arteriosus (DA). This may be secondary either to PPHN or to obstruction of aortic arch (eg, interrupted aortic arch [IAA] and severe aortic coarctation).
Although failure to increase PO2 with 100% O2 is greatly indicative of cyanotic CHD, some neonates with severe PD do not demonstrate elevation in PO2. In such babies, continuous positive airway pressure (CPAP) may be useful in the differentiation of pulmonary from heart disease (Figures 10.1). Application of 8 to 10 cm H2O CPAP with 100% O2 for a period of 10 to 15 minutes via a face mask is likely to show improvement in PO2 (> 10 torr) in babies with PD, whereas no change or a decrease may be seen in cyanotic CHD infants.10,11
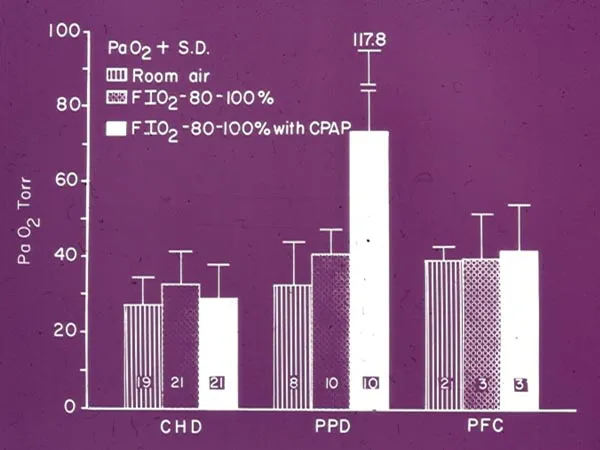
Figure 10.1. Bar graph demonstrating usefulness of CPAP in the diagnosis of cyanotic infants. In the congenital heart disease (CHD) and PFC groups, there was no increase in arterial PO2 following administration of 100% oxygen along with CPAP. In the PD group, while there was no increase in PO2 after 100% O2, the PO2 increased with CPAP. The PO2s are shown as mean + SD. The number of infants studies in each group is marked within bar. The data are derived from Reference 11.
Diagnosis of Specific Type of CHD
Having recognized a baby with a cardiac problem, additional designation of type of CHD is based on scrutiny of pulmonary blood flow (PBF) on a posterior–anterior view of a chest x-ray: (1) decreased pulmonary vascular markings (Figure 10.2); (2) increased pulmonary vascular markings (Figures 10.3 and 10.4); and (3) severe pulmonary venous congestion (Figure 10.5). High-quality chest x-ray with deep inspiration and without patient rotation is obligatory to accomplish precise evaluation of pulmonary vascular markings.
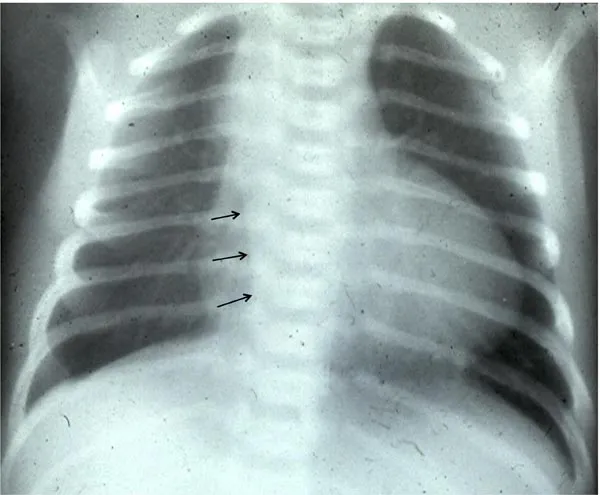
Figure 10.2. Chest x-ray of an infant with decreased PBF. Mild enlargement of the heart with markedly decreased PBF may be seen. Note right aortic arch (small arrows), which suggests that the diagnosis is likely to be TOF.
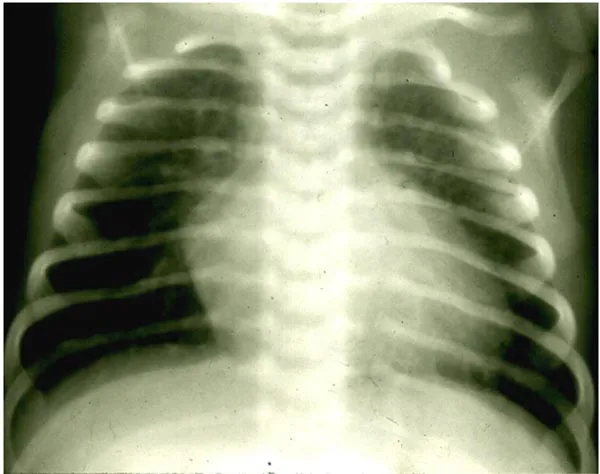
Figure 10.3. Chest x-ray of an infant with increased PBF. Mild enlargement of the heart with moderately increased PBF is seen. On further studies, this infant was demonstrated to have TGA with intact ventricular septum.

Figure 10.4. Chest x-ray of an infant with increased PBF. Severe enlargement of the heart with markedly increased PBF is seen. On further studies, this infant was diagnosed to have HLHS.

Figure 10.5. Chest x-ray of an infant with pulmonary venous congestion. A picture of severe pulmonary venous congestion with no significant enlargement of the heart is seen.
Decreased Pulmonary Vascular Markings
The most frequently encountered CHDs in this group are shown in Table 10.3. Diagnosis of infants with decreased PBF can be made by analysis of the ECG (Figure 10.6). Advanced knowledge of ECG interpretation/understanding is not needed for this approach. Calculation of axis (mean frontal plane vector), which is learned in medical school, is su...
Table of contents
- cover
- Title
- Copyright
- Dedication
- Contents
- Contributors
- Foreword
- Preface
- Acknowledgments
- Abbreviations
- Section I - Perinatal Circulation
- Section II - The Fetus
- Section III - Ethics
- Section IV - Changes in Oxygen Saturations at Birth and Pulse Oximetry Screening
- Section V - Diagnosis and Management
- Section VI - Individual Cardiac Defects
- Section VII - Cardiomyopathies
- Section VIII - Hypertension
- Section IX - Conclusions
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Perinatal Cardiology: A Multidisciplinary Approach by P. Syamasundar Rao, Dharmapuri Vidyasagar, P. Syamasundar Rao,Dharmapuri Vidyasagar in PDF and/or ePUB format, as well as other popular books in Medicine & Cardiology. We have over 1.5 million books available in our catalogue for you to explore.