The first comprehensive resource on transseptal catheterization.Although the transseptal technique was described half a century ago, it has remained essentially unchanged. Recent advances in cardiac electrophysiology and left heart interventions have led to renewed interest in the technique as a means of delivering modern therapeutic interventions.Until now, the knowledge required for safely gaining access to the left atrium to perform catheter ablation for atrial fibrillation or other interventions has existed only in original publications and review articles. This textbook brings all of the relevant information about this technique under one cover, with top experts in each area addressing anatomy, indications, transseptal puncture, visualization technologies, interventional devices, challenging cases, complications, and emerging tools. Electrophysiologists and interventional cardiologists will find Transseptal Catheterization and Interventions invaluable for their work. For teachers and trainees, it will be a welcome teaching tool and resource.Transseptal Catheterization and Interventions was listed by the American Journal of Cardiology as one of the "Good Books in Cardiovascular Disease in 2010". - American Journal of Cardiology Vol. 107, Issue 8, Pages 1250-1251Transseptal left heart catheterization is here to stay. It already plays an important role in the repertoire of both interventional cardiologists and clinical electrophysiologists, and it will play an increasingly important role in the future.
eBook - ePub
Transseptal Catheterization and Interventions
- 256 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Transseptal Catheterization and Interventions
About this book
Information
Topic
MedicineSubtopic
Cardiology1
HISTORY OF
TRANSSEPTAL CATHETERIZATION
GREGORY K. FELD, JOHN ROSS JR.
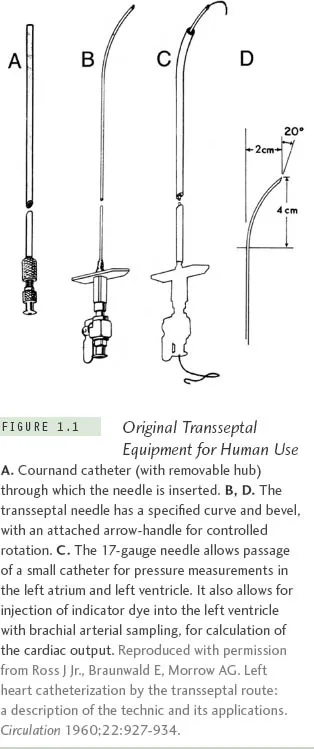
Transseptal left heart catheterization, originally developed in experimental animal studies and then later in humans, was reported in 1959 by John Ross Jr, MD, at the National Institutes of Health (NIH).1-4 It was first used to measure left heart pressures as a diagnostic method and later as a research tool to study left heart dynamics in human diseases such as heart failure, heart valve dysfunction, and hypertrophic obstructive cardiomyopathy.4,5,* In 1960, the needle used for transseptal catheterization (Figure 1.1) was slightly modified with a smaller needle tip by Edwin Brockenbrough, MD, a trainee in the NIH cardiovascular research program, for use with a larger catheter passed percutaneously by the Seldinger method.7 Subsequently the procedure became widely used as a diagnostic method to assess left atrial and left ventricular pressures in both adult and pediatric patients with valvular and congenital heart disease who were being considered as candidates for surgical repair procedures.8-10 With the developments of right heart, balloon, and thermodilution (Swan-Ganz) catheterization to estimate left atrial pressures11 and retrograde left ventricular catheterization, transseptal catheterization became less widely practiced in the 1970s and early 1980s, except in those centers performing procedures, such as mitral balloon valvulotomy, which require transseptal puncture.
During the 1980s, however, at a time when clinical cardiac electrophysiology was primarily a diagnostic specialty, the use of electrical fulguration for atrioventricular (AV) node ablation, septal accessory pathway ablation, and ventricular tachycardia ablation was described,12-13 rapidly advancing cardiac electrophysiology into an interventional specialty. Fortunately, considering the limitations of high-energy shocks for ablation, including the high failure rates and risks of complications from this technique,12-13 radiofrequency energy for catheter ablation was described.14 This led to an explosion in the use of catheter ablation to cure a variety of cardiac arrhythmias, including AV reentry,15-16 AV nodal reentry,17 atrial flutter,18-19 atrial tachycardia,20and ventricular tachycardia.21
In many cases, however, the successful application of radiofrequency energy via catheter for curative ablation required access to the left atrium and left ventricle. This was particularly true for left-sided accessory pathways,15-16 left ventricular tachycardia,21 atrial fibrillation and atypical atrial flutter.22 While often this could be accomplished by retrograde arterial catheterization across the aortic and mitral valves, usually from the femoral artery or rarely from the radial artery, in many cases easier access could be achieved by a transseptal catheterization approach. Thus, for the treatment of a variety of supraventricular and ventricular tachyarrhythmias there was a gradual resurgence in the use of transseptal catheterization in the field of interventional cardiac electrophysiology, beginning in the 1980s; this use increased dramatically in the 2000s as ablation of atrial fibrillation became widely practiced.
Thus, in the cardiac electrophysiology laboratory, transseptal catheterization has become particularly useful for obtaining access to the left atrium for radiofrequency catheter ablation of left-sided accessory pathways in patients with Wolff-Parkinson-White syndrome and refractory supraventricular tachycardia,23-25 in the occasional patient with failed right-sided slow or fast pathway ablation for AV nodal reentrant tachycardia,26-27 in those with failed right-sided AV node ablation for refractory atrial fibrillation,28 and in those with left ventricular tachycardia in whom access to the left ventricle is required for both mapping and ablation.29-30 Large numbers of transseptal catheterization procedures have been performed at numerous institutions worldwide over the last several decades, including many in electrophysiology laboratories, with very high success and very low complication rates,31 even if performed on an outpatient basis.32 The most serious potential risks from transseptal catheterization include cardiac or aortic perforation with pericardial effusion and tamponade, which may require percutaneous pericardial catheter drainage and, occasionally, surgical intervention.
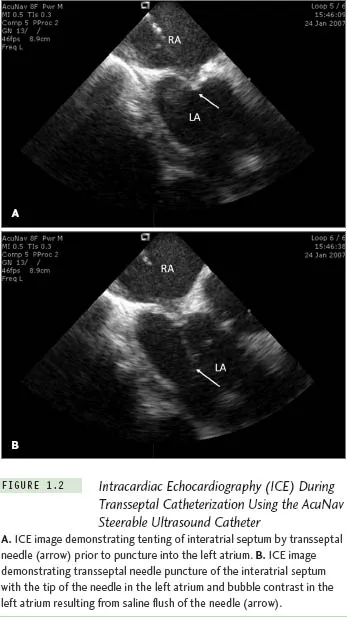
While the technique of transseptal catheterization remains largely unchanged since it was originally described and modified,14 several new technologies have made the approach considerably easier and potentially less risky, and are routinely employed today in many clinical electrophysiology laboratories. These new technologies include transesophageal echocardiography,33 now largely replaced by intracardiac echocardiography (ICE),34-37 to guide transseptal puncture, transseptal puncture performed using radio-frequency energy applied to a modified transseptal needle (NRG RF Transseptal Needle, Baylis Medical Company, Inc, Montreal QC, Canada), or use of a needle-tipped guidewire (SafeSept Transseptal Guidewire, Pressure Products, Inc, San Pedro, CA) passed through a standard Brockenbrough transseptal needle into the left atrium through a variety of pre-shaped transseptal sheaths (Fast-Cath, St. Jude Medical, Inc, St. Paul, MN). With the use of ICE, typically performed with a steer-able 8 F or 10 F intracardiac ultrasound catheter (AcuNav, Siemens Medical Solutions USA, Inc, Malvern, PA), contrast injection to stain the septum is no longer required, since micro-bubbles in the saline flush provide adequate echo-contrast to ensure successful left atrial access, reducing the risk of cardiac perforation with the transseptal needle (Figure 1.2). The radiofrequency transseptal needle38 and the needle-tipped guidewire further reduce the risk of inadvertent needle perforation of the left atrial lateral wall or roof during transseptal catheterization. For ablation of left-sided accessory pathways, a numbered series of transseptal sheaths (eg, SL1, SL2 [Daig Corp, Minnetonka, MN]) with different lengths of the distal-shaped segment was developed that, when extended just beyond the sheath, position the ablation catheter at specific locations around the mitral valve annulus (Fast-Cath, St. Jude Medical, Inc, St. Paul, MN).
With the recognition that electrical isolation of the pulmonary veins with radio-frequency catheter ablation may cure atrial fibrillation,39 an entirely new procedure in interventional cardiac electrophysiology was launched in the late 1980s, namely the ablation of atrial fibrillation. This approach required transseptal catheterization of the left atrium and, in most cases, double transseptal catheterization (Figure 1.3) because both a circular mapping catheter and an ablation catheter need to be introduced into the left atrium to ensure successful isolation of the pulmonary veins. This can be accomplished either by performing two separate transseptal punctures33-37 or a single transseptal puncture40 through which an ablation catheter is guided either by ICE or fluoroscopy after withdrawing the sheath (through which the initial puncture was made) back into the right atrium while retaining a guidewire in the left atrium. Once the ablation catheter is passed through the transseptal puncture into the left atrium, the retained sheath can be passed over the guidewire back into the left atrium, through which the circular mapping catheter can then be deployed in the left atrium for mapping the pulmonary veins. Both approaches may be guided by ICE, and recent advances in 3-D echo may further enhance success and reduce the risks of the procedure. Studies suggest that long-term complications are similar with either approach, and while the single transseptal puncture approach may result in patency of the puncture site for a longer period of time than the double transseptal puncture approach, closure eventually occurs with either approach.41
Another aspect of transseptal catheterization that has evolved with the advent of atrial fibrillation ablation has been the use of intensified anticoagulation regimens for prevention of thromboembolic events, including maintaining an activated clotting time (ACT) >350 seconds during abla...
Table of contents
- Cover
- Title
- Copyright
- Dedication
- Contents
- Contributors
- Foreword
- Preface
- Chapter 1
- Chapter 2
- Chapter 3
- Chapter 4
- Chapter 5
- Chapter 6
- Chapter 7
- Chapter 8
- Chapter 9
- Chapter 10
- Chapter 11
- Chapter 12
- Chapter 13
- Chapter 14
- Chapter 15
- Index
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Transseptal Catheterization and Interventions by Ranjan Thakur, Andrea Natale, Ranjan Thakur,Andrea Natale in PDF and/or ePUB format, as well as other popular books in Medicine & Cardiology. We have over 1.5 million books available in our catalogue for you to explore.