Acute Coronary Syndrome: Urgent and Follow-up Care is a must-read for all those involved in the care of ACS, including EMS, nurses, advanced practice providers as well as physicians. This book not only reviews the causes of ACS, but also provides evidence-based acute and follow-up treatment recommendations that incorporate the perspectives of all those involved in the care of these patients. Epidemiology, pathophysiology, and outcomes of acute coronary syndromes The role of EMS in the triage of the ACS patient Evaluation and treatment of the ACS patient in the emergency department Pharmacologic management of the ACS patient Follow-up care of the ACS patient The role of the team in carrying out successful guideline-driven care
eBook - ePub
Acute Coronary Syndrome
Urgent and Follow-up Care
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Acute Coronary Syndrome
Urgent and Follow-up Care
About this book
Information
Topic
MedicineSubtopic
CardiologyCHAPTER 1
Epidemiology
Garrett Ruth, MD, Garrett Brown, MD, Eileen Handberg, PhD, ARNP-BC, and R. David Anderson, MD, MS
Acute Coronary Syndrome: Urgent and Follow-up Care © 2017
Joseph S. Alpert, Lynne T. Braun, Barbara J. Fletcher, Gerald Fletcher, Editors-in-Chief, Cardiotext Publishing, ISBN: 978-1-935395-94-2
Joseph S. Alpert, Lynne T. Braun, Barbara J. Fletcher, Gerald Fletcher, Editors-in-Chief, Cardiotext Publishing, ISBN: 978-1-935395-94-2
INTRODUCTION
Acute coronary syndrome (ACS) is a term used for any condition brought on by sudden, reduced blood flow to the heart. The diagnosis of an ACS includes a spectrum of disease presentation ranging from unstable angina, to non-ST-segment elevation myocardial infarction (MI), to ST-segment elevation MI. It is usually associated with coronary artery disease (CAD), most commonly atherosclerosis. All of these conditions can progress to advancing disease and eventually lead to death. In many developed countries, heart disease is the leading cause of morbidity and mortality. Although the overall mortality rate in the United States has declined, CAD claims more than one-third of the deaths in persons over 35 years of age. Population data have shown that 1 of 2 men and 1 of 3 women in the United States will present with some symptomatic CAD in their lifetime. As the population gets older, the prevalence of CAD steadily increases. The 2010 Heart Disease and Stroke Statistics review reported that 17.6 million people in the United States have CAD.1
CARDIOVASCULAR DISEASE RISK FACTORS
CAD is localized to the heart but is a part of a larger group of atherosclerotic diseases classified as cardiovascular disease. Cardiovascular disease refers to atherosclerosis that affects the entire arterial circulation, not just the coronary arteries. There are many manifestations including stroke, transient ischemic attack, angina, MI, and claudication. Cardiovascular disease is present in various populations but has an increased incidence in groups with specific risk factors. A growing trend of comorbidities such as obesity, hypertension, tobacco use, and cholesterol levels all contribute to the increasing overall burden of cardiovascular disease.
The prevalence of obesity (body mass index [BMI] ≥30 kg/m2) has doubled in the years 1980 to 2008, and over 2.8 million deaths per year are attributed to being overweight (BMI ≥25 kg/m2) or obese. In 1980, population statistics showed 5% of men and 8% of women were classified as obese. In 2008, 10% of men and 14% of women across the world were considered obese. It has also been shown that America has the highest prevalence of overweight (62%) and obese (26%) individuals (Figure 1.1).2
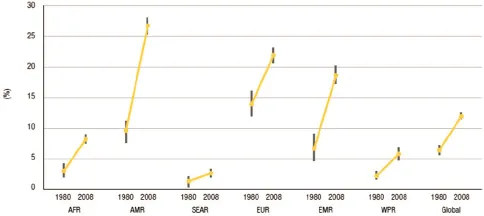
Figure 1.1
Change over time in mean BMI by WHO region, 1980 to 2008.
AFR = African region; AMR = Americas region; BMI = body mass index; EMR = Eastern Mediterranean region; EUR = European region; SEAR = South-East Asia region; WPR = West Pacific region.
(Source: Reprinted with permission from World Health Organization. World Health Statistics. 2012.)
Population studies have shown that, worldwide, 40% of people older than age 25 have hypertension, and the number of people with elevated blood pressure has increased from 600 million in 1980 to a billion in 2008. This number will continue to grow and has been estimated to be 1.6 billion by the year 2025. Elevated blood pressure not only contributes to cardiovascular deaths (45%) but also has been found to be a contributing factor to more than 51% of stroke deaths worldwide.
Mean cholesterol levels have improved globally since the 1980s with the advent of statins, but still remain elevated in some developed countries. These decreases have been shown to be most significant in the high-income countries (mean decrease from 5.62 to 5.19 mmol/L) compared with low-income countries (4.46–4.20 mmol/L) and middle-income countries (4.91–4.7 mmol/L). Despite these improvements, 39% of the world’s population has elevated cholesterol, with percentages >50% in some higher-income countries.
Smoking and tobacco use in the United States have declined over the past 25 years. Whereas in 1965 >40% of the population smoked, in 2010, this has decreased to 19.3%.2 This is the fourth lowest rate of tobacco use among the countries involved in the Organization for Economic Cooperation and Development, behind Iceland, Sweden, and Mexico. From the most recent data, countries that still have >25% of residents who smoke include Greece, Ireland, Hungary, Estonia, Spain, and Turkey.3
EPIDEMIOLOGY OF CORONARY ARTERY DISEASE
In a 2009 report that used National Health and Nutrition Examination Survey (NHANES) data, prevalence of MI was compared by gender in individuals of middle age (35–54 years) from the periods 1988 to 1994 and 1999 to 2004.4 Overall, both studied periods demonstrated greater prevalence in men. However, the trend showed a decrease in men (2.5–0.7 from 1988 to 1994 and 2.2–1.0 from 1999 to 2004) and an increase in women. The NHANES report noted that data were self-reported for MI and angina and likely underestimated the actual prevalence of advanced heart disease.
Two large postmortem studies have shown a reduction in the incidence of anatomic coronary heart disease (CHD) over time. In one particular report, over 2500 autopsies were performed from the years 1979 to 1994 recording the prevalence of clinical anatomic CHD. The patients were aged 20 to 60 years, and results showed a decrease from 42% to 32% in men and 29% to 16% in women when the specific periods 1979 to 1983 and 1990 to 1994 were compared.5 However, in ages >60 years, there was no change in prevalence. In another study, over 3800 autopsies were performed on U.S. military personnel who died of combat or unintentional injuries in a 10-year span from 2001 to 2011. This particular cohort had an average age of 26 years and comprised 98% men. Results showed that CHD only was present in 8.5% of subjects.6 This was a drastic difference in those studied in previous wartime years such as the Korean War in the 1950s (77%) and the Vietnam War in the 1960s (45%).
Using the Framingham study, both initial subjects and offspring have been studied, allowing recording of statistics in relation to CAD and events detailing both recognized and silent MI, angina pectoris, unstable angina, and sudden cardiac death.7–9 From these data, the following conclusions were made:
a) In people at age 40, the lifetime risk of developing CAD is 49% in men and 32% in women. For those who reach age 70, the lifetime risk is 35% in men and 24% in women.
b) The incidence of total coronary disease rises with age; however, women lag behind men by 10 years. Related to more serious outcomes such as sudden cardiac death and severe CAD, women lag behind by over 20 years, but these differences begin to attenuate with advancing age.7 For example, comparing subjects aged 35 to 64 years with those aged 65 to 94 years, the incidence of CAD doubles in men and triples in women.
c) In the premenopausal population, extensive coronary disease and sudden cardiac death are rare. However, following menopause, the incidence and severity of coronary disease increases, with a threefold risk compared with women of the same age who are premenopausal, owing to the cardioprotective effects of estrogen.7
d) In the population below 65 years of age, the annual incidence of all coronary events in men (12 per 1000) more than equals the rate of all other atherosclerotic cardiovascular events combined (7 per 1000); in women, it equals the rate of the other events (5 per 1000). Beyond 65 years of age, coronary disease still predominates. Coronary events comprise 33% to 65% of atherosclerotic cardiovascular events in men and 28% to 58% in women.
e) In women under age 75 years, the initial symptom of coronary disease is more likely to be angina pectoris than MI.8 Men typically have angina following MI (66%), while women who have angina have relatively uncomplicated disease or stable angina. MI includes a large portion of men in whom only 20% of infarctions are preceded by long-standing angina. If the infarction is silent, that number decreases even further.8,9
f) With the addition of medications for atherosclerotic disease such as stat...
Table of contents
- Cover
- Title Page
- Copyright
- Contents
- About the Editors-in-Chief
- About the Authors
- Preface
- Abbreviations
- Section 1: Acute Coronary Syndromes
- Section 2: Acute Coronary Syndromes: Urgent Care
- Section 3: Acute Coronary Syndromes: Follow-up Care
- Index
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Acute Coronary Syndrome by Eileen Handberg, A. Richard Anderson, Eileen Handberg,A. Richard Anderson in PDF and/or ePUB format, as well as other popular books in Medicine & Cardiology. We have over 1.5 million books available in our catalogue for you to explore.