This user-friendly workbook provides adults with obsessive compulsive disorder (OCD), the tools they need to move beyond their disorder using Acceptance and Commitment Therapy (ACT) and it also serves as compact text for clinicians/practitioners to use with clients suffering from OCD at any point in treatment.
The workbook offers readers hands-on ACT and Exposure Response Prevention (ERP) skills for taming disturbing obsessions and filling the gap of where one stands and where one wants to go. Dr. Zurita provides evidence-based exercises to guide adults through the process of ACT. This includes learning to step back from one's thoughts and memories, opening up to all types of unwanted thoughts and feelings, paying attention to the physical world, observing one's thoughts and feelings, getting rid of barriers to values-based living, and developing consistent patterns of values-based behavior.
Written from the office of a full-time therapist in a simple, uncomplicated, and unpretentious manner, this workbook will be useful for all clients suffering from OCD and for the therapists who work with them.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
This first part gives you the basics to start where you are. It’s about unpicking the stories we tell ourselves about thinking, how our mind works, and how we relate to fear. You’ll learn what OCD is, the many ways in which it’s reinforced, and the different themes it comes up with.
Your mind is very good at playing tricks, and learning how it does this is liberating!
1 Obsessions Are the Norm!
I know that we don’t know each other and that we haven’t met, but if I were next to you and we were going to start talking about OCD, I would share with you a memory I have of one of those warm and humid summer nights in Bolivia, my country of origin.
I was driving back to Santa Cruz, one of Bolivia’s main cities, after a long camping trip. I was sweaty because of the high temperature and elevated humidity of the tropical weather. I could feel the hot air slapping my face, moving through my nose every time I breathed in and breathed out. My face was shiny with perspiration. I was listening to music, as I usually do on a long trip. Despite the heat, I was feeling refreshed from my time in the forest, thinking lightly about conversations I had, and ready to go to sleep wrapped in the clean sheets on my bed.
I was driving at a regular speed on the freeway when, suddenly, the white lights of a truck driving toward me on the opposite side of the road made me suck in a deep breath. Instantly, I saw in my mind this awful scene of being hit by the truck, my car pushed to the side of the road, my body covered in blood, and me dying quickly. The image was so clear and vivid that I began to hyperventilate and sweat even more. I gripped the wheel really hard with both of my hands. And then the truck passed. The experience lasted only seconds, but it felt like an eternity to me. I pulled over, still hyperventilating. I couldn’t shake the image in my mind – it was very clear and very real.
The image I created in my mind has never left. In fact, it pops up from time to time, even when I’m not driving. And at times my mind tells me that this image “proves that I’m going to die young.” I sometimes get anxious when driving next to a big truck, and I hold the wheel really hard with both hands. This image is so real that, no matter where I am, who I’m with, what I’m doing, it can show up any time.
Looking back, it’s clear that I had an intrusive thought and a panic attack. And because this image continues to show up and is sticky, I can classify it as an obsession. Obsessions are thoughts or images that are unwanted, repetitive, scary, hard to let go of, and come with a strong sense of urgency; they also include urges or impulses, which is a way of describing an intense bodily sensation (like washing hands) paired with an unwanted thought (like My hands are covered in germs!). In this workbook, we’ll use the terms “obsessions” and “intrusive thoughts” interchangeably when referring to “thoughts, images, and urges.”
Let me clarify right away that obsessions are not a personality trait, a symbol of your unconscious mind, or a hidden intention. Intrusive thoughts can be confusing because they vary in degrees of bizarreness and incongruence with your character and your values, so they can range from being ego-syntonic or benign to ego-dystonic or ultra-weird. In other words, some obsessions – the ego-syntonic ones – are more consistent with a person’s view of the world, feel natural, and are not distressing. The opposite goes for ego-dystonic ones.
If we think about the “weirdness” of thoughts, or thinking in general, as a naturally occurring phenomenon that everyone’s mind has, we may see it as a continuum:
Let’s take a look at how this frame applies to some random intrusive thoughts:
Images of having sex with another person than your partner
Fears of people stealing your knowledge
Images of punching a person
Doubts about your existence being real
Fears of losing control
Random images of blood in a curtain
Fears about your partner cheating on you
How about your own intrusive thoughts? Think about the obsessions you have been having over the last month and mark an X under the category where it fits best.
Intrusive thought
ultra–weird
weird
a bit weird
not weird at all
But, again, it’s important to keep in mind that all obsessions are content generated by our mind, and at their core, they’re annoying, aggravating, and, as little dictators, demand you do something about them right away.
Is It Only You?
There’s been a lot of research studies around obsessions. Don’t worry, I won’t go into all of them. But here are just a few studies that are important for you to be aware of.
Rachman and de Silva (1978), Salkovskis and Harrison (1984), and Radomsky and his colleagues (2014) assessed how obsessions show up among adults in the United States and college students in 13 countries across six different continents. Guess what they found? Obsessions are part of the brain chatter in everyone’s daily life, whether we are diagnosed as having OCD or not.
Here is a take-home message from those studies: everyone has bizarre thoughts.
For instance, Melissa, a 45-year-old saleswoman, has chosen to work part-time to spend quality time with her kids. On a Sunday afternoon, she is lying down on the couch with her 7-year-old son, and her arm, by accident, touches her kid’s genital area. At that moment, Melissa has the thought, “Did I like it? Am I a pedophile? Am I going to abuse my kid?” She quickly moves off the couch and sits apart from her son.
I don’t know the annoying obsession your mind comes up with, but you’re not alone, you’re not crazy, and you’re not defective. It’s absolutely normal to have weird, unwanted, scary, or disturbing thoughts. They’re part of being human, part of what our normal mind does – whether we have OCD or not.
Our minds are constantly coming up with theories, hypotheses, problems to solve, thoughts about the past, images, patterns, wishful thoughts, revenge contemplations, romantic memories, worries, stories, doubtful thoughts, and so on, nonstop and without taking any breaks, vacations, or holidays. Don’t believe me? Try the next exercise.
Exercise: Watching Your Mind
Get a timer and set it for 3 minutes, and in those 3 minutes watch the stuff that your mind comes up with. Just do your best to notice all the things your mind conjures up. When the alarm sounds, jot down the thoughts and images you had:
What did your mind do? Every time I watch my mind, it never surprises me the amount of blah-blah-blah it comes up with. Sometimes that blah-blah-blah is interesting, fun, and insightful, and other times it’s a massive stream of images, random thoughts, and a bunch of nonsensical noise. Our busy minds also come up with intrusive thoughts; that’s the norm, and not the exception.
You may be wondering, “If everyone has all types of thoughts, including dark obsessions, how do I have OCD?” We’ll answer that in the next chapter.
2 If Obsessions Are Normal, What About OCD?
What starts obsessive-compulsive disorder? How does a person go from having a disturbing thought to spending hours dealing with OCD?
To start, let’s think for a moment about Theo, a 26-year-old art graduate student who loves history classes. Theo is fascinated by modern European history, loves to read all types of books, watch movies, and debate about them.
One afternoon, while Theo was listening to his teacher lecturing about the Cold War, he noticed a weird sensation while swallowing, as if he wasn’t swallowing on the right side of his throat and there something was wrong with it. His mind quickly had thoughts about how important swallowing is for eating, drinking, talking, etc., and he started panicking about having a problem with his swallowing. Theo swallowed multiple times, faster, slower, and when doing so, he noticed that at times his swallowing felt a bit normal.
He tried to continue listening to the history lecture, and then, when swallowing again, he noticed that there was a sensation of dryness, so this time he put his hands on his throat while swallowing and checked what was wrong – he even tried to stop swallowing for a minute to see if his swallowing went back to normal. Theo went to the bathroom, turned on the water faucet, put his hand under it, and brought it to his mouth, hoping that extra water would help his swallowing and the weird sensation that something was wrong. Theo went back to class and moved his tongue inside his mouth multiple times to help his swallowing. But while he found at times his swallowing was okay, he continued to have thoughts about something being potentially wrong with his swallowing and it being an indication of chronic illness.
Later that night, Theo was careful how much he was talking to his girlfriend, checked the amount of saliva he had, how his swallowing felt when eating and snacking, drank more water than usual and refused to drink a beer with his dad (as they usually did), and when going to sleep he searched “swallowing problems” online. Theo found all types of information, from chronic medical conditions like cancer and autoimmune disorder to transitory ones like a cold. Theo just had a medical check a month ago, and the doctors didn’t find anything of medical concern. He didn’t have any other symptoms of flu, cold, sore throat, or any other related condition, but despite knowing all that, Theo couldn’t let go of the thought “Something is wrong with my swallowing.” The next day, Theo decided to skip breakfast just in case coffee would make his swallowing worse and to monitor the dryness of his throat to compare whether he had more saliva the moment before.
Here is a connection that Theo’s brain made: a weird sensation with swallowing equals danger, distress, and anxiety. Keeping Theo’s experience in mind, let’s unpack it to answer two questions. What starts OCD? What maintains it?
How Does an OCD Episode Start?
Theo’s OCD struggles started with not-so-weird unwanted thoughts that he couldn’t let go of. “Is there something wrong with my saliva? Do I have a serious medical condition that I don’t know about?” Theo managed the discomfort that came along with those obsessions by doing all types of checking.
And even though it seems natural that any person would check whether they have a medical condition or not, what’s different is that Theo was very bothered by these obsessions. He was in distress, couldn’t continue with his day, couldn’t dismiss those thoughts. He often checked the amount of saliva he had, changed the pace of his swallowing, researched online, and checked the symptoms of other illnesses. Every time Theo did any of those behaviors, he felt a bit better momentarily about the quality of his swallowing. But it was only a matter of time until the obsession about something being wrong with his swallowing showed up again in Theo’s mind. And he tried to manage it, again and again, using the same short-lived strategies.
Theo kept doing those checking behaviors for a single reason: to get rid of the obsession. He was determined to minimize the impact of the thought, making sure there was nothing wrong with his swallowing. All those behaviors are called compulsions. And the tricky part with compulsions is that, while they can calm you down quickly, they only calm you down until get triggered again.
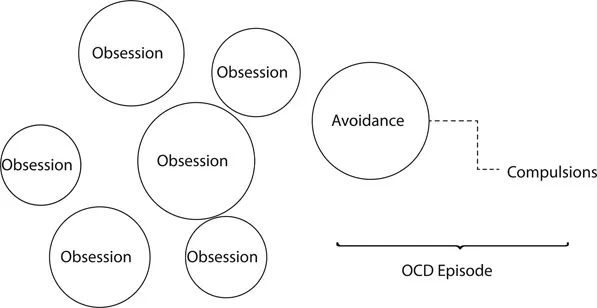
Figure 2.1 is a graphic to explain how Theo went from having an obsession to an OCD episode, and how it starts.
Figure 2.1 From an obsession to an OCD episode.
Theo went from having an obsession to having an OCD episode because his brain quickly learned that one way to let go of the distress, fear, and panic of the obsession is by doing a compulsion. Who wouldn’t? Acting based on the fear, distress, panic, and agony that comes with obsessions is like a scratching an itch – there is a sense of relief that comes right away. That’s how OCD starts.
Compulsions and avoidant behaviors – things you do right away to avoid the discomfort, distress, and anxiety that comes with intrusive thoughts – work immediately. And any person struggling with these very sticky obsessions will quickly develop patterns of compulsions – doing different types of checking, rituals, and so forth – or different types of avoidance.
So now you know how your mind works when triggered; in the next chapters, you’ll learn more about compulsions and avoidant behaviors.
3 What Keeps OCD Going?
OCD doesn’t keep going on its own. OCD keeps getting bigger and bigger, worse and worse, because compulsions and avoidant behaviors work – but only in the short term. They alleviate your distress, take the edge off the fear, but they last only seconds. And that’s why you keep doing them, over and over.
Let me go into nerdy behavioral land for a bit, because this information is important to understand: how do you go from one OCD episode into another one? Behaviorally speaking, doing compulsions and avoidant behaviors “negatively reinforces” the cycle of an OCD episode. If you recall, one of the first associations that Theo’s brain made was that a weird sensation when swallowing equals danger. Next, Theo’s brain learned that, when doing compulsions and avoidant behaviors, he co...
Table of contents
Cover
Half Title
Title Page
Copyright Page
Dedication Page
Contents
List of Figures
List of Tables
List of Exercises
Introduction
Part I Getting to Know Your Mind: A Pattern-Making Machine
Part II What Would ACT Do for You?
Part III The Trilogy That Makes Your Life Miserable
Part IV Facts and Fantasy About Getting Rid of Obsessions
Part V Learning to Date Your Mind
Part VI Shift, Shift, Shift … Shift Your Moves!
Part VII Designing Your Life and Living Your Life
Part VIII Making W.I.S.E. M.O.V.E.S.
Part IX Unpacking Blocks for Making W.I.S.E. M.O.V.E.S.
Part X Moving Forward
Departing Words
Appendices
About the Author
Bibliography
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Living Beyond OCD Using Acceptance and Commitment Therapy by Patricia E. Zurita Ona in PDF and/or ePUB format, as well as other popular books in Personal Development & Abnormal Psychology. We have over 1.5 million books available in our catalogue for you to explore.