Sex and gender in biomedicine are innovative research concepts of theoretical and clinical medicine that enable a better understanding of health and disease, evidence-based knowledge, effective therapies, and better health outcomes for women and men. Gender medicine, which focuses on the impact of gender on human physiology, pathophysiology, and clinical features of diseases, stimulates new ways of doing research by considering sex and gender at all levels of investigation, from basic research into gene polymorphisms to health behavior. New research questions have been put forward that focus not on differences per se but on the developmnetal path of these differences. In this book, contributions from the fields of neuroscience, addiction research, and organ transplantation exemplify concepts, approaches, methods and results in the field of gender medicine.
eBook - ePub
Sex & Gender in Biomedicine
Theories, Methodologies, Results
- 126 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Sex & Gender in Biomedicine
Theories, Methodologies, Results
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineGender issues in living organ donation: medical, social, and ethical aspects
1 Abstract
The gender-disparity hypothesis for living kidney transplantation has been discussed for more than 20 years. It states that women donate kidneys more frequently than men, but fewer women than men receive organs. Our investigation aims at a) the quantitative verification of the gender-disparity-hypothesis in four European countries and b) the qualitative and ethical analysis of possible causes. Our quantitative analysis is based upon data for Germany, the Netherlands, Belgium and Austria provided by Eurotransplant for a five year period (2003–2007). On the recipient side, the higher number of men could be explained by statistically taking into account the sex-ratio for end stage renal disease. On the donor side, there is a significant difference between expected and observed numbers of women serving as donors in all four countries. Parents as living donors are the most important group to explain the deviation. Fathers donate to their children significantly less often and mothers more often than one would expect according to epidemiological data. To explore reasons behind these behavioural differences, we conducted and analysed focus group discussions in Austria, Germany and the Netherlands to gather information about attitudes and moral positions. Following the assumptions of the two-moralities debate, we found differences between men and women in their argumentation concerning (1) the formal structure of decision making and judgment (2), the role of the family for moral argumentation, and (3) the assessment of public institutions such as the state, the market and the medical system. Our findings indicate that gender related roles (and expectations) have a great impact on framing moral issues in organ transplantation while general moral attitudes are rather similar between men and women. We finally discuss consequences for clinical practice as well as for further research.
2 Introduction: is there a gender aspect in organ donation?
Organ donation has complex medical, social, and ethical aspects. In this paper, we address sex and gender issues in organ transplantation, precisely, differences between men and women donating or receiving an organ. In many Western countries, about twice as many women as men donate a kidney. This fact, however, is still often neglected in medical and ethical overviews of organ transplantation. For the purpose of this paper, we focus on living organ donation, particularly on kidney transplantation: first, most evidence is available with regard to living organ donation (LOD). Though one can also observe a difference in sex of donors in post-mortem transplantation, this is yet not well investigated.1 Second, in most countries, only the number of living kidney transplantations (LKD) is high enough to detect sex and gender related differences while living liver and lung transplantations are still too rare for gaining evidence with respect to an imbalance in the sexes. First, we will present statistical findings substantiating significant differences in the men/women ratio on the donor and on the recipient side; secondly, we will consider social and psycho-moral aspects of organ donation which interact with medical practice. Against this background, we will, thirdly, present socio-empirical data from focus group discussions with male and female potential donors exploring socio-cultural and moral factors for gender differences in donation. Finally, we discuss why and how gender issues should be addressed in the clinical setting.
3 Quantitative socio-demographical and medical data
A variety of quantitative differences between men and women on several levels can be found in LKD. First and foremost, if we compare absolute numbers and sex proportion between donors and recipients we constantly observe a deviation from the normal population sex ratio (49% male vs. 51% female). (See table 1). However, it is necessary to analyse each side separately. On the recipient side, we statistically observe over time steady and over country rather stable differences – on average 37–41% are female patients and 59–63% male without high variations between different countries. (See table 1, first column, for an overview see also (2)) On the donor side, we observe differences in the sex ratio in various countries, too (see table 1, second column), but in this case there are much higher variations between different countries. In Germany, for instance, 61% of all living donors are female whereas only 39% are male. In Switzerland, the disparity is even more pronounced: 65% of living organ donors are female while only 35% are male (3). In the USA, Kayler et al. (4) as well as recent UNOS (5) data show the same trend. In contrast, in Great Britain (6) and Norway (7) the sex ratio of donors is less pronounced but has still not reached sex equality with regard to donors or recipients. Iran seems to be a special case. Here, the sex ratio on the donor side is reversed: more men than women are donors. This reversed effect on the donor side is explained by special legal and economic frameworks. In Iran (8) donors in living unrelated donation get paid by the state as well as by the family of the recipient. The same trend was reported in recent studies showing that in the case of (illegal) commercialisation of organ donation (e.g. in Latin America and East-Asia), men sell their organs much more often than women (9). Also, German men are more willing to donate when offered a hypothetical financial incentive (10).
Table 1: Comparison of the total numbers of living kidney donations with respect to sex ratio in various countries with established living kidney donor programmes.
Country | f : m recipient | f : m donors | LKD in% of total kidney transplantation | Source |
Germany | 39 : 61% | 61 : 39% | 20% | Eurotransplant (2003–2007) (11) |
USA | 39 : 61% | 59 : 41% | 44% | UNOS (2009) (5) |
Switzerland | 36 : 64% | 65 : 35% | 18% | (1993–2003) (3) |
UK | 41 : 59% | 53 : 47% | 39% | UK Transplant (2007–2008) (6) |
Norway | 37 : 63% | 58 : 42% | 40% | (1985–2002) (5) |
Iran | 37 : 63% | 22 : 78% | 95% | (8) |
Comparing four European countries, all of them members of Eurotransplant2, we found an interesting pattern of ratio of men-women on the donor as well as on the recipient side. (See graph 1a and 1b). To this purpose, we analysed statistical data available for Germany, Netherlands, Belgium, and Austria for a period of time between 2003 and 2007. In these countries the lumped sum of a 5-years period was large enough for substantial statistical analysis of LKD (in Austria N=232; in Belgium N=150; in Germany N=2507; and in the Netherlands N=1360). In an analogous study to Kayler et al. (4) we considered the sex ratio of each country’s population as well as the sex differences in end stage renal disease (ESRD) for the statistical analysis (mean comparison test with Unixstat). ESRD is the main reason for kidney transplantation, the epidemiology of ESRD shows a statistically highly relevant deviation between men and women. ((4), For details on the calculation see also (2)). Out of 100 cases of ESRD 61.8 are men and 38.2 are women. This sex difference in ESRD was taken into account when calculating the potential number of recipients of kidney transplantations.
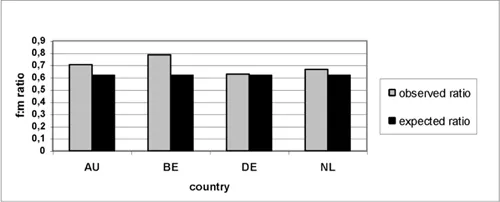
Graph 1a: Women/men ratio in relation to observed and expected recipients’ numbers in living kidney transplantation in Austria (AU), Belgium (BE), Germany (DE) and the Netherlands (NL) Data provided by Eurotransplant 2003–2007 (N=4249). The slight differences between observed and expected sex ratio in all four countries are statistically non-significant.
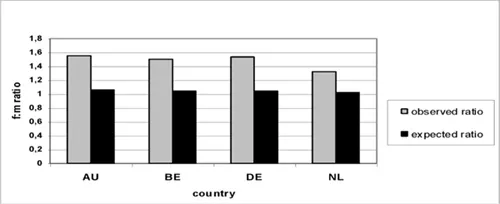
Graph 1b: Women/men ratio in relation to observed and expected donors’ numbers in living kidney transplantation in Austria [AU: p <0.005], Belgium [BE: p<0.05,] Germany [DE: p<0.00005], The Netherlands [NL: p<0.00005] (data provided by Eurotransplant for 2003–2007) (N=4249)). The deviation between observed and expected sex ratio in all four countries are statistically significant.
In graph 1a and 1b we have summarised the results of a comparison of observed and expected ratio of female and male recipients and donors in four countries. On the recipient side a statistical analysis (Chi-square test, N=4249 for all four countries) did not reveal statistically significant differences, while on the donor side there are significant differences between observed and expected female-male ratio in all four countries. Our results are mainly in line with findings for other countries (e.g. (12, 14)) showing that the gender ‘effect’ on the donor and recipient side has different reasons. Thus, they raise different concerns. In our study, the differences between men and women on the recipient side, in line with the study of Oien et al. (7) for Norway, can be explained by epidemiological facts (concerning ESRD and population ratio). However, the high impact of ...
Table of contents
- Cover
- Title
- Copyright
- Table of Contents
- Preface
- Preface
- Editorial
- Sex and gender in biomedicine: promises for women and men
- Gender issues in living organ donation: medical, social, and ethical aspects
- Sex, gender, and the brain – biological determinism versus socio-cultural constructivism
- The brain between sex and gender – women and men from a neuroscientific perspective
- Sex and gender in addiction research and therapy
- Contributors
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Sex & Gender in Biomedicine by Ineke Klinge,Claudia Wiesemann, Ineke Klinge, Claudia Wiesemann in PDF and/or ePUB format, as well as other popular books in Medicine & Medical Theory, Practice & Reference. We have over 1.5 million books available in our catalogue for you to explore.