eBook - ePub
Advances in Neurolaryngology
- 180 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Advances in Neurolaryngology
About this book
Volume 85 in the series 'Advances in Oto-Rhino-Laryngology' contains a combination of our current understanding of neurolaryngological anatomy, physiology, pathology and management options. The content of 'Advances in Neurolaryngology' is divided into four sections, namely Anatomy and Physiology, Examination and Investigation, Conditions and Therapeutic Options, and Fresh Perspectives and the Future. All the chapters have been written by internationally recognized experts in their field who provide a valuable update on the latest research. Interesting aspects of many of areas in the basic science, diagnostics and treatment options in Neurolaryngology are provided. New approaches when evaluating (for example, Chapter 2 – Visual Neurolaryngology) or managing and understanding other subsets of patients (see Chapter 16 – The Hidden Anatomy of Opera Singers) make this publication both current and fascinating! This publication is aimed at all healthcare workers who are involved in the management of patients with neurolaryngological conditions namely ENT surgeons, neurologists, radiologists, electrophysiologists, speech and language therapists, respiratory physicians and their respective trainees.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Conditions and Therapeutic Options
Published online: November 9, 2020
Prasad VMN, Remacle M (eds): Advances in Neurolaryngology. Adv Otorhinolaryngol. Basel, Karger, 2020, vol 85, pp 59–67 (DOI: 10.1159/000496491)
______________________
Vocal Fold Immobility: An Algorithm for Treating Glottal Insufficiency
Vaninder K. Dhillona Lee M. Akstb
aDivision of Laryngology and Endocrine Head and Neck Surgery, Department of Otolaryngology-Head and Neck Surgery, Johns Hopkins University School of Medicine, Suburban Hospital, Bethesda, MD, USA; bDivision of Laryngology, Department of Otolaryngology-Head and Neck Surgery, Johns Hopkins University School of Medicine, Johns Hopkins Hospital, Baltimore, MD, USA
______________________
Abstract
The objectives of this chapter are to discuss the factors involved in the decision-making algorithm of an appropriate intervention for glottal insufficiency. Management strategies not only depend on the etiology, history, symptoms, size of glottal gap on visualization, but also on patient goals and expectations. The goal of this chapter is to organize the management of glottal incompetence for patients and providers, supported by an evidence-based approach.
© 2020 S. Karger AG, Basel
Introduction
Glottal insufficiency occurs when there is incomplete vocal fold closure. Patients who incur glottal insufficiency may have neurophysiologic impairment such as vocal fold paralysis or paresis or reduced motion secondary to anatomical impairment such as stenosis. Vocal fold atrophy can lead to change in muscle tone of the true vocal fold, and this can also lead to incomplete closure. The negative impact on both voice and swallowing determines what treatment options should be considered. Symptoms can include decreased projection, increased vocal effort, early vocal fatigue, and risk for aspiration pneumonia.
The algorithm to navigate surgical and nonsurgical treatment options include factors related to the etiology of glottal incompetence, potential for eventual recovery of glottal closure, size and configuration of the glottal gap, degree of patient voice and swallow handicap, and patient comorbidity.
This chapter will enumerate an algorithm that can be used when deciding which patients might be candidates for one treatment option over another in the management of glottal insufficiency. Literature around outcomes of treatment will be reviewed, and the thought process that helps to guide decision-making for patients with glottal incompetency will be examined.
Evaluation
Evaluation is the first step in deciding the appropriate treatment for glottal insufficiency. The history, including the etiology and symptoms associated with glottal insufficiency, followed by direct visualization of the glottal gap, will help in the assessment of a patient’s laryngeal function. The assessment of a patient’s laryngeal function and the impact that insufficiency has on the patient’s voice and swallow helps guide appropriate management.
History
Symptoms
The symptoms surrounding patients with glottal insufficiency are unique to each patient. A patient’s vocal demand, use of voice as well as underlying comorbidities must be taken into account when assessing changes in voice and swallow. Examples of how voice may change include increased breathiness, change in conversational projection, increased fatigue or effort. From a swallow standpoint, there may be dysphagia to solids and liquids, or coughing and choking with solids and/or liquids. Weight loss or pneumonia may result for those who have incomplete closure and are unable to compensate, while others may not have any dysphagia symptoms. There may be symptoms of a weak or less effective cough, and an increased sensation of phlegm in the throat that is poorly cleared.
Onset of symptoms, including the acuity or chronicity and the progressive or stable nature of the symptoms, is information that can provide clues as to etiology of the glottal incompetency and may inform further workup and treatment decisions. Things to inquire in good history taking include history of recent upper respiratory infection, recent surgeries including neck, spine, or chest surgery that may put the recurrent laryngeal nerve at risk, and a history of trauma to the neck. A good neurology workup may be necessary if there are symptoms associated with changes in gait, balance, or tremor. Glottal insufficiency in the absence of vocal fold paralysis may be a part of other neurodegenerative disorders that may provide insight for an underlying primary neurologic process.
Visualization of the Glottis
Laryngeal examination in the form of laryngoscopy and/or stroboscopy is the primary means of assessing size of the glottal gap and glottal insufficiency. There is a correlation between voice symptoms and size of glottal gap [1]. From a symptom perspective, the size of the gap is often more predictive of patient complaints than is the etiologyof the gap [2]. The size of the glottal gap can influence the algorithm for treatment.
Stroboscopy allows frame-by-frame evaluation of glottal closure as compared to fiberoptic laryngoscopy and provides a more accurate assessment of the size of the glottal gap, allowing for direct evaluation of the impact of reduced glottal closure on the physiology of voicing.
Radiologic imaging is an important component of working up glottal insufficiency secondary to direct visualization of vocal fold paralysis on examination [3]. If the etiology of the vocal fold paralysis is unknown, computed tomography scanning along the course of the recurrent laryngeal nerve is required to assess for occult lesions [4]. Vocal fold paralysis associated with palatal weakness, deviation of the tongue with protrusion, or other cranial nerve findings may be secondary to a vagal or more proximal weakness, and imaging should include the skull base and brainstem to evaluate for lesions along the course of the vagus nerve. With isolated vocal fold paresis, patients should be followed, and if motion impairment is progressive, then imaging is warranted [4, 5]. For patients with dysphagia or where there is a concern for aspiration, a modified barium swallow is important to help in identification of the problem and institution of a management plan for aspiration risk.
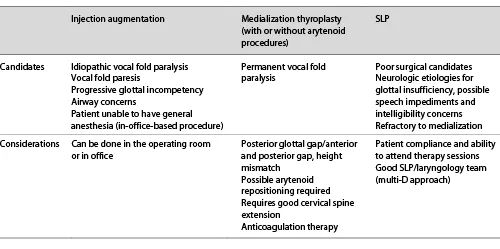
Table 1. Treatment options for glottal insufficiency
Further testing including laryngeal electromyography has not been shown to have a definite diagnostic role in vocal fold paralysis or paresis [6].
Speech Language Pathology and Other Subspecialty Evaluations
Speech language pathology (SLP) is a crucial part of the workup for patients with glottal insufficiency, from both a diagnostic but also therapeutic standpoint. The assessment of functional contributions of voice and swallow concerns allows for improved behavioral treatments with voice and swallow therapy [7]. If glottal insufficiency may be related to a neurodegenerative diagnosis, then a neurology evaluation is important. A full neurologic workup allows for improved diagnosis, treatment prognostic information that can affect treatment decisions made by the patient and the otolaryngologist [8].
Treatment Options and Medical Decision Making
When deciding between the main treatment options for glottal insufficiency, it is important to identify the etiology of the insufficiency, patient symptoms, the size of the glottal gap, patient goals and expectations, and the achievability of the treatment plan. The main treatment options for glottal incompetency include vocal fold augmentation/medialization, and behavioral therapy with SLP. In turn, vocal fold augmentation/medialization can be done either through injection laryngoplasty or framework surgery such as thyroplasty with or without arytenoid repositioning [9].
The following section will incorporate the medical decision making process for each treatment option. A summary of treatment options can be seen in Table 1. The decision making process must consider whether additional closure will be helpful as well as the patient’s ability to tolerate intervention. Some questions to consider may be:
•Will medialization be helpful?
•How much medialization is required? Unilateral or bilateral?
•What is the etiology of the glottal insufficiency?
•What is the patient’s tolerance for an office-based procedure?
•What is the patient’s candidacy, relative to comorbidity, for an operating room procedure?

Fig. 1. Glottal insufficiency in vocal fold scarring and/or atrophy.
Consideration of intervention can include coexistence of other issues that might lead to voice or swallowing handicap along with the size of the glottal gap. In general, the degree of benefit to a vocal fold medialization/augmentation is in direct proportion to the size of the gap being closed. There are many examples, whereby there may be primary vocal fold changes including scar and atrophy, and the size of the glottal gap may be small. The benefit of the medialization may be different, and perhaps less effective, as compared to a patient with a larger glottal gap such as vocal fold paralysis.
Furthermore, mobility of the vocal fold is important when considering medialization options. In patients with unilateral vocal fold paralysis (UVFP) who may have a large posterior gap, a framework procedure that includes arytenoid repositioning may be more beneficial over an injection approach that largely addresses only the membranous vocal folds. Mobile vocal folds with reduced closure or coordination may benefit from a bilateral procedure with small amounts of material on each side to achieve a straighter edge (Fig. 1). For patients with the possibility of progressive vocal fold motion impairment or vocal fold atrophy, it is important to have a treatment option that takes into account the airway. The airway may change either now or in the future. In this setting, augmentation should be conservative or might incorporate plans for tracheotomy.
Functional issues should be addressed with SLP. Comorbid exacerbating factors – deconditioning, reduced breath support, rapid fatiguability as with multiple sclerosis (MS), reduced motor coordination as with P...
Table of contents
- Cover Page
- Front Matter
- Anatomy and Physiology
- Examination and Investigation
- Conditions and Therapeutic Options
- Fresh Perspectives and the Future
- Author Index
- Subject Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Advances in Neurolaryngology by V.M.N. Prasad,M. Remacle, Patrick J. Bradley,Patrick J., Bradley,Vyas M.N., Prasad,Marc, Remacle in PDF and/or ePUB format, as well as other popular books in Medicine & Neurology. We have over 1.5 million books available in our catalogue for you to explore.