- 68 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Atrial Fibrillation in Practice
About this book
This book provides a clear, concise, management-orientated approach to atrial fibrillation. It also provides a useful and practical guide to the issues relating to this common cardiac problem, to improve the care and treatment of these patients.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
1. Epidemiology and importance
Introduction
Epidemiology
Incidence and prevalence
Clinical implications and importance
Does asymptomatic atrial fibrillation carry the same degree of risk as the symptomatic form?
Atrial fibrillation in the community
Atrial fibrillation in hospital practice
Atrial fibrillation and the patient
Introduction
Until fairly recently, atrial fibrillation (AF) was often regarded as an innocuous cardiac rhythm disorder, where patients could simply be treated with some digoxin and left well alone. Nothing could be further from the truth – AF is now recognized as a very important cause of mortality and substantial morbidity from heart failure, stroke and thromboembolism. Many patients with AF suffer from reduced exercise capacity as well as poor quality of life.
Indeed, AF is encountered in a wide variety of clinical settings. It may, for example, be discovered incidentally in an asymptomatic patient, it may develop in a patient who merely has a chest infection, fever or it may be found in a patient with a ventricular rate of 200 beats per minute who is too dizzy or lightheaded to stand up! While many are asymptomatic, many patients with AF have a wide variety of cardiorespiratory-presenting symptoms and clinical features, including syncope, heart failure and stroke. Many patients may require long term treatment with potent antiarrhythmic and anticoagulant drugs, which may have important pharmacological interactions and adverse effects.
With the increasing age of the general population, AF is likely to become an even greater public health problem. Current perceptives of AF are summarized below.
Atrial fibrillation – the present
• Recent randomized controlled trials have clearly established the value of antithrombotic therapy in preventing stroke and thromboembolism in AF.
• Clinicians have recognized the limitations of simply treating AF with digoxin.
• Considerable advances have been made in the management of AF as more is understood about the underlying pathophysiology and electrophysiology of this condition.
• Better appreciation of the different clinical subtypes of AF, that is, paroxysmal (recurrent), persistent and permanent AF allows definition of objectives and strategies of management.
Epidemiology
The prevalence of AF varies widely around the world and varies according to the population studied. Much of the clinical epidemiology of AF is also based on data from predominantly Caucasian populations, and information on AF in non-Caucasian populations is scarce. Current perspectives on the epidemiology of AF are summarized below and in Table 1.1.
The risk of AF is well recognized to increase with age and with underlying heart disease. For example, the risk of AF has been found to be associated with increasing age, male sex, heart failure, valve disease, coronary heart disease, diabetes and hypertension. In the Cardiovascular Health Study, 57% of people with AF had clinical cardiovascular disease, and with AF had sub-clinical cardiovascular disease, and a further 35% had sub-clinical cardiovascular disease (being defined as abnormal findings on echocardiography or carotid ultrasound). Conversely, AF is uncommon in infants, children and healthy young adults.
Epidemiology of atrial fibrillation
• AF is the most common sustained cardiac rhythm disorder (Figure 1.1).
• AF is more common with increasing age, and is associated with common cardiovascular and non-cardiovascular diseases.
• Common cardiac causes of AF include hypertension, valve disease and ischaemic heart disease.
• Common non-cardiac causes of AF include thyroid disease, chest disease and intrathoracic pathology.
• Much of the clinical epidemiology of AF pertains to Caucasian populations. In Afro-Caribbeans, hypertension is likely to be the most common cause, while in Indo-Asians, ischaemic heart disease is the most common.
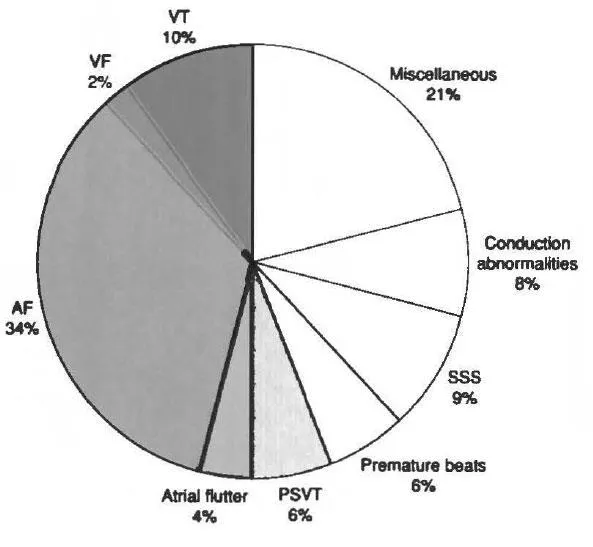
Hospitalizations for cardiac arrhythmias. VT – ventricular tachycardia; VF – ventricular fibrillation; SSS – sick sinus syndrome; PSVT – paroxysmal supraventricular tachycardia; AF – atrial fibrillation. Adapted from Bialy et al. J Am Coll Cardiol 1992; 19: 41 A.
Incidence and prevalence
The prevalence of AF approximately doubles with each advancing decade of age, from 0.5% at age 50-59 years to almost 9% at age 80-89 years (see Figure 1.2). AF is also becoming significantly more prevalent, increasing in men aged 65-84 years from 3.2% in 1968-1970 to 9.1% in 1987-1989, an increase which is not explained by an increase in risk factors such as valve disease or myocardial infarction. It is estimated that more than one-half (56%) of people with AF are aged >75.
White (n=213) | Black (n=10) | Asian (n=22) | |
|---|---|---|---|
Age in years: | 75.3 (11.0) | 73.1 (12.1) | 62.4 (15.5) |
mean (SD) | |||
Past medical history | |||
None | 19 | 1 | 2 |
Ischaemic heart disease | 53(24.9%) | 1 | 10 (45/5%) |
Valvular heart disease | 11 | 0 | 2 |
Ischaemic and valvular heart disease | 5 | 0 | 0 |
Thyroid disease | 16 (7.5%) | 0 | 0 |
Cardiomyopathy | 0 | 0 | 2 |
Heart failure | 39 | 3 | 4 |
Hypertension | 45 (21.1%) | 5 (50%) | 1 |
Cerebrovascular disease | 29 (13.6%) | 0 | 2 |
Diabetes mellitus | 22 | 0 | 2 |
Other | 8 | 0 | 2 |
Applying age-specific prevalence rates to the population structure of England and Wales allows England and Wales specific estimates to be derived. Using this approach, the overall prevalence in England and Wales is 1.1%, rising to 6.1% in people aged >65, and to 8.6% in people aged >75.
AF is more common in men than women and over one-half (56%) of people with AF are aged >75. For example, in the largest UK study from Newcastle, the prevalence was 10% in men and 5.6% in women aged >75. Studies that have sub-divided AF into chronic and paroxysmal suggest that about one-quarter is paroxysmal, with the latter being younger and with a higher proportion (approximately 50%) being ‘lone’ AF.
In the Cardiovascular Health Study, the reported incidence for men aged 65 to 74 and 75 to 84 were 17.6 and 42.7 per 1000 person years respectively and for women, 10.1 and 21.6. Framingham study results were similar, but with smaller differences between men and women. On the basis of 38-year follow-up data from the Framingham Study, men had a 1.5-fold greater risk of developing AF than women after adjustment for age and predisposing conditions.
Clinical implications and importance
Key issues regarding the clinical implications and importance of AF are summarized in the box. The main burden of AF management rests with primary care clinicians as many do not present to hospital. Issues hence relate towards better detection and appropriate investigation of such patients.
Clinical implications and importance of AF
• AF represents a frequent problem not only for hospital physicians but also for primary care physicians.
• Most of AF appears to be managed by general practitioners, and in fact, only a third of patients with AF have ever been admitted to hospital
• Surveys of AF in the community and among ...
Table of contents
- Cover
- Title Page
- Copyright Page
- Dedication
- Contents
- 1 Epidemiology and importance
- 2 Aetiology
- 3 Pathophysiology and electrophysiology
- 4 Clinical features
- 5 Investigations
- 6 Non-drug management
- 7 Drug management
- 8 Management strategies
- 9 Antithrombotic therapy
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Atrial Fibrillation in Practice by Gregory Y H Lip in PDF and/or ePUB format, as well as other popular books in Medicine & Audiology & Speech Pathology. We have over 1.5 million books available in our catalogue for you to explore.