The revised guide to the diagnosis, management, and treatment of blood disorders and cancer in children
Children with blood disorders and cancer are a unique population that require specialized diagnostic considerations and management. The Handbook of Pediatric Hematology and Oncology has been designed to provide clinicians of all levels with practical guidance through an up-to-date algorithmic approach to these conditions. Assembled by a team of experts from the world-class Children's Hospital & Research Center Oakland, this updated third edition:
- Presents up-to-date management and treatment guidelines for the most common pediatric blood disorders and malignancies
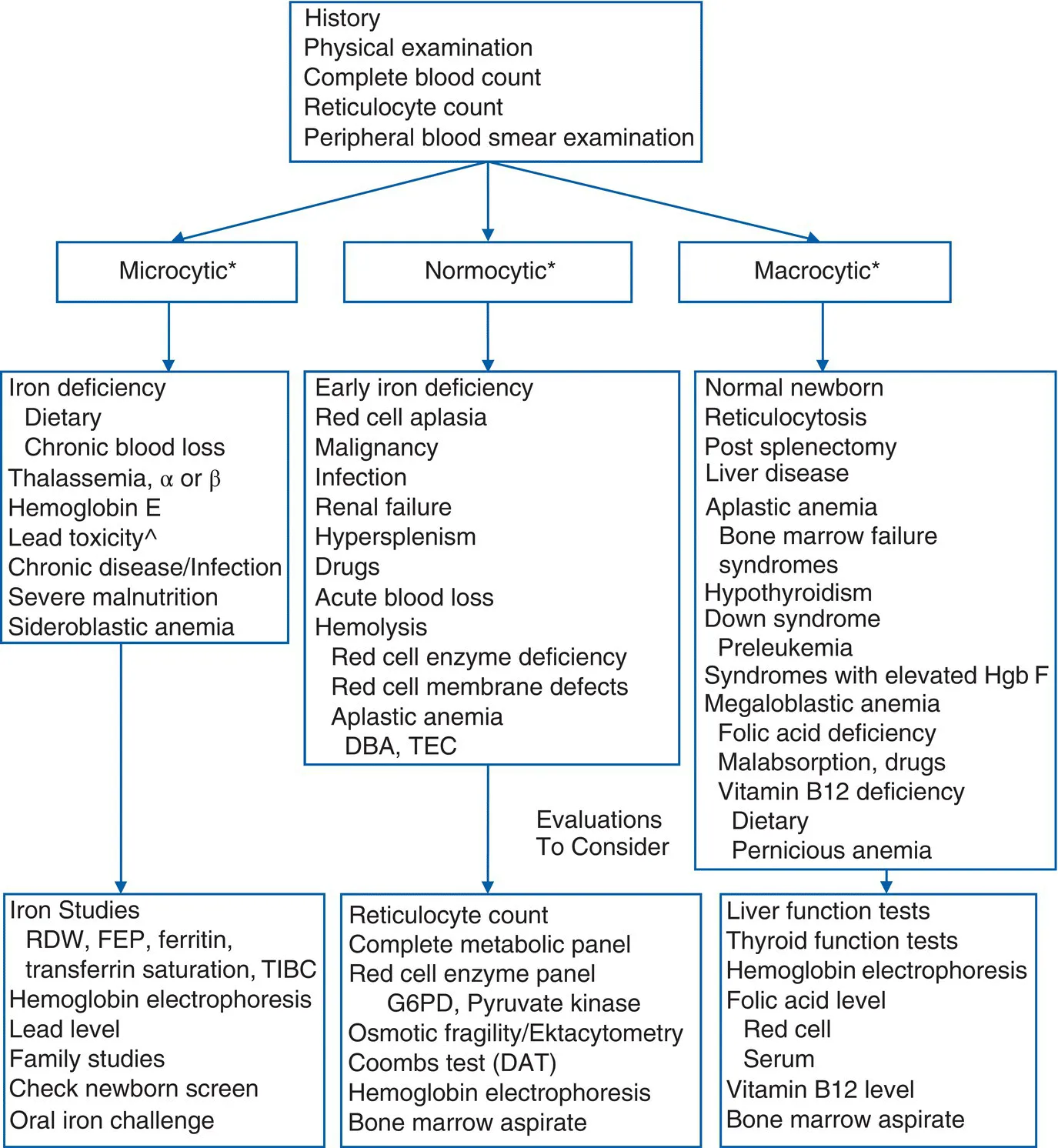
- Provides an updated algorithmic approach for the diagnosis and management of the most common conditions and suggested readings
- Utilizes rapid-referral tables containing visual representations of symptoms, lab findings, differentials, and treatment guidance
- Incorporates case studies covering different hematologic and oncologic conditions, such as hemolytic anemia, sickle cell disease, hemophilia, neuroblastoma, and sarcomas of the soft tissue and bone
- Includes a useful formulary that lists chemotherapy agents, dosing, mechanism of action, pregnancy category, indications, and side effects
- Covers transfusion medicine, stem cell transplantation, management of central venous catheters, acute pain management, oncologic emergencies, and chemotherapy basics
With its direct guidance and portable design, the Handbook of Pediatric Hematology and Oncology: Children's Hospital & Research Center Oakland, Third Edition, will prove an invaluable resource to medical students, trainees and residents, pediatric hematology and oncology nurses, pediatricians, and early-career providers in pediatric hematology/oncology.