Robert Baran, MD Honorary Professor, University of Franche-Comté; Nail Disease Center, Cannes, France Dimitris Rigopoulos, MD, PhDProfessor of Dermatology-Venereology, School of Health Sciences, National and Kapodistrian University of Athens, Athens, Greece
Chander Grover, MD, DNB, MNAMS Professor of Dermatology, University College of Medical Sciences and GTB Hospital, Delhi, India
Eckart Haneke, MD Dermatology Practice Dermaticum, Freiburg, Germany; Centro de Dermatología Epidermis, Instituto CUF, Porto, Portugal; Kliniek voor Huidziekten, Universitair Ziekenhuis, Ghent, Belgium; Department of Dermatology, Inselspital, University of Bern, Bern, Switzerland
A succinct guide to treatment options, both medical and surgical, for both disorders and injuries of the nail.
From reviews of the first edition: "This is a book about nail therapies that is relevant clinically while remaining a manageable size. It would be a useful tool for all clinicians managing nail disease, from the trainee to those embarking on a clinic dedicated to nail disease." Br J Dermatol
Contents: Anatomy and physiology of the nail unit * Psoriasis * Onychomycosis * Novel and emerging pharmacotherapy and device-based treatments for onychomycosis * Lichen planus * Onychotillomania (onychophagia, habit tic, median canaliform onychodystrophy) * Eczema * Acrodermatitis continua of Hallopeau * Herpes simplex (herpetic whitlow, herpetic paronychia) * Acute paronychia * Chronic paronychia * Warts * Yellow nail syndrome * Onycholysis * Nail fragility and beautification * Nail prostheses * Nail pigmentation * How to prevent and treat chemotherapy-induced nail abnormalities * Intralesional nail therapies * Drug side effects on the distal phalanx * Classical nail surgery and removal of the proximal nail fold * Surgery of some common nail tumors * Nail surgery complications * The painful nail * Radiation and the nail
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
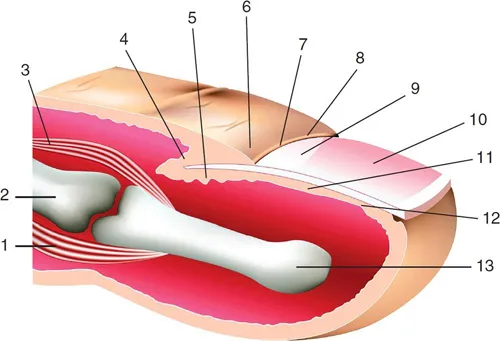
The nail plate is the permanent product of the nail matrix. Its normal appearance and growth depend on the integrity of several components such as the tissues surrounding the nail, or perionychium, the bony phalanx that contribute to the nail apparatus or nail unit (Figure 1.1).
Figure 1.1 Anatomy of the nail apparatus: 1. flexor tendon; 2. middle phalanx; 3. extensor tendon; 4. eponychium; 5. nail matrix; 6. proximal nail fold; 7. cuticle; 8. lateral nail fold; 9. lunula; 10. nail plate; 11. nail bed; 12. hyponychium; 13. terminal phalanx.
The nail is a semi-hard horny plate covering the dorsal aspect of the tip of the digit. The nail is inserted proximally in an invagination practically parallel to the upper surface of the skin and laterally in the lateral nail grooves. This pocket-like invagination has a roof, the proximal nail fold, and a floor, the matrix from which the nail is derived.
The matrix extends approximately 6 mm under the proximal nail fold, and its distal portion is only visible as the white semi-circular lunula. The general shape of the matrix is a crescent concave in its posteroinferior portion. The lateral horns of this crescent are more developed in the great toe and located at the coronal plane of the bone. The ventral aspect of the proximal nail fold encompasses both a lower portion, the matrix, and an upper portion (roughly three-quarters of its length) called the eponychium.
The germinal matrix forms the bulk of the nail plate. The proximal element forms the superficial third of the nail, whereas the distal element covers its inferior by two-thirds.
The ventral surface of the proximal nail fold adheres closely to the nail for a short distance and forms a gradually desquamating tissue, the cuticle, made of the stratum corneum of both the dorsal and the ventral side of the proximal nail fold. The cuticle seals and, therefore, protects the ungual cul-de-sac from harmful environmental agents.
The nail plate is bordered by the proximal nail fold, which is continuous with the similarly structured lateral nail fold on each side. The nail bed extends from the lunula to the hyponychium. It presents with parallel longitudinal rete ridges.
The nail bed, in contrast to the matrix, has a firm attachment to the nail plate. Therefore, its avulsion produces a denudation of the nail bed. Colorless but translucent, the highly vascular connective tissue containing glomus organs transmits a pink color through the nail.
Distally, adjacent to the nail bed, the hyponychium, an extension of the volar epidermis under the nail plate, marks the point at which the nail separates from the underlying tissue.
The distal nail groove, which is convex anteriorly, separates the hyponychium from the fingertip.
Circulation of the nail apparatus is supplied by two digital arteries that course along the digits and send out branches to the distal and proximal arches.
The sensory nerves to the dorsum of the distal phalanx of the three middle fingers are derived from fine oblique dorsal branches of the volar collateral nerves. Longitudinal branches of the dorsal collateral nerves supply the terminal phalanx of the fifth digit and the thumb.
Among its multiple functions, the nail provides counterpressure for the pulp that is essential to the tactile sensation involving the fingers and for the prevention of distal wall tissue produced after nail loss of the great toenail.
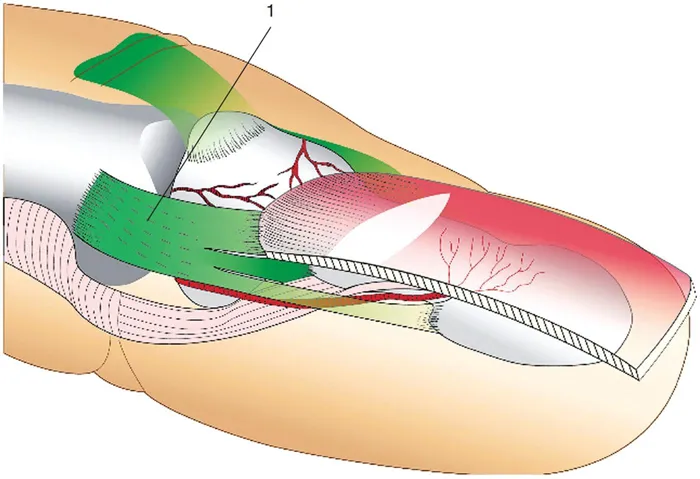
The nail is a musculoskeletal appendage as a part of a functional unit that is comprised of the distal bony phalanx and several structures of the distal interphalangeal joint extensor tendon fibers and the collateral ligaments. All these form the enthesis (Figure 1.2). This organ is the bony insertion point of the ligaments, the tendons, and the articular capsules. It is composed of both
•Soft tissue (ligaments, tendons, and their fibrocartilages)
•Hard tissue (calcified fibrocartilage, the immediately adjacent bone of the underlying trabecular network)
Figure 1.2 Entheses of the nail apparatus with (1) dorsal expansion of the lateral ligament at the distal interphalangeal joint (Guerro’s ligament).
Histological images confirm the link between the different structures.
Histology permits recognition of the nail matrix and nail bed that have no granular layer, in contrast to the upper ventral aspect of the proximal nail fold called eponychium and the hyponychium.
The hard keratin of the nail lies perpendicularly to the nail growth axis and parallel to the surface of the nail plate.
Fingernails grow continuously on an average of 0.1 mm per day (3 mm per month). Toenails form over a period of 12–18 months.
The nail unit is in some respects comparable to a hair follicle sectioned longitudinally and laid on its side. The epithelial components of hair follicle and nail apparatus are differentiated epidermal structures that may be involved jointly in several ways, such as lichen planus and alopecia areata.
•Only the nail matrix produces the nail plate.
•No bone, no nail.
•Knowledge of growth rate is often helpful in establishing the disease onset.
•Entheses play an important role in nail anatomy.
FURTHER READING
De Berker DAD, André J., Baran R. (2007) Nail biology and nail science. Int J Cosm Sci; 29: 241–275.
McGonagle D., Tan A. L., Benjamin M. (2008) The biomechanical link between skin and joint disease in psoriasis and psoriatic arthritis: what every dermatologist needs to know. Ann Rheum Dis; 67: 1–9.
Morgan A. M., Baran R., Haneke E. (2001) Anatomy of the nail unit in relation to the distal digit. In and Krull E. A., Zook E. G., Baran R., Haneke E. (eds). Nails Surgery. A Text Atlas. Lippincott William Wilkins, Philadelphia PA, 1–28.
2
Psoriasis
Dimitris Rigopoulos
Psoriasis is presented in various forms involving different parts of the nail unit, as shown in Table 2.1.
Table 2.1
Signs of Psoriasis
Matrix involvement
Nail bed involvement
Fold involvement
Pits, trachyonychia
Onycholysis
Paronychia
Leukonychia
Oil-drop sign
Nail plate disorders
Nail fragility
Splinter hemorrhages
Dystrophic alterations
Subungual hyperkeratosis
Beau’s lines
Onychomadesis
Mottled redness in the lunula
Pits
These are the commonest signs of psoriasis. They are mainly seen on fingernails. Nail disease most typically affects the dominant hand thumbnail and then the other nails that are most associated with hand function. Incidence of fingernail pitting increases with the total duration and severity of the disease. They are deeper than those in alopecia areata and also more numerous, and they can be transient or in some cases, long lasting. The presence of more than 20 pits suggests a psoriatic cause of the nail dystrophy, while more than 60 pits per person are unlikely to be found in the absence of psoriasis. There is no sex predilection while concerning age; patients over 40 years are affected twice as often as those under 20 years. It is also notable that several pits can result in trachyonychia-like appearance of the nails. When the psoriatic lesion affects a wider area of the nail matrix, transverse grooves (onychomadesis) are formed in the same way as pits. They are due to involvement of the proximal part of the nail matrix, resulting in abnormal cornification and presence of parakeratotic corneocytes in the nail plate. These cells, as they are loosely attached, drop out, leaving punctuate depressions on the nail plate (resembling a thimble), which correspond to the pits (Figure 2.1). The parakeratotic cells that remain are visible like scales within the pits.
Figure 2.1 Pitting on the proximal nail plate associated with distal onycholysis.
Subungual Hyperkeratosis
This is due to the inflammation of the hyponychium and the distal nail bed and the hyperplasia of the epi...
Table of contents
Cover
Half Title
Title Page
Copyright Page
Contents
Preface
Contributors
1. Anatomy and physiology of the nail unit
2. Psoriasis
3. Onychomycosis
4. Novel and emerging pharmacotherapy and device-based treatments for onychomycosis
5. Lichen planus
6. Onychotillomania (onychophagia, habit tic, median canaliform onychodystrophy)
18. How to prevent and treat chemotherapy-induced nail abnormalities
19. Intralesional nail therapies
20. Drug side effects on the distal phalanx
21. Classical nail surgery and removal of the proximal nail fold
22. Surgery of some common nail tumors
23. Nail surgery complications
24. The painful nail
25. Radiation and the nail
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Nail Therapies by Robert Baran, Dimitris Rigopoulos, Chander Grover, Eckart Haneke, Robert Baran,Dimitris Rigopoulos,Chander Grover,Eckart Haneke in PDF and/or ePUB format, as well as other popular books in Medicine & Dermatology. We have over 1.5 million books available in our catalogue for you to explore.