Forensic neuropathology is an important specialty within forensic pathology. In addition to traumatic brain injury in the adult and child, forensic neuropathologists must also consider the role of natural disease within the forensic setting such as cerebrovascular disease, as well as neurotoxicology. Focusing on difficulties that arise in the medico-legal context, the chapters include techniques for the post-mortem examination of the brain and related structures. Forensic pathologists, neuropathologists, general pathologists, clinical forensic specialists as well as neuroscientists, neurologists and neurosurgeons will all find useful information. In addition, members of the legal profession have found this an important reference work.
Chapters have been extensively revised and new content includes
- Updates on pathological aspects of head injury including infant head injury with ocular pathology
- Clinical aspects of head injury and spinal injury including a new chapter on neuroradiology
Reviews of the First Edition
This outstanding book is unique. Well-illustrated with high-quality colour photographs and line drawings, it reads well. Strongly recommended for trainees in histopathology, neuropathology, paediatric pathology, and forensic pathology, as well as for consultants practising in these fields.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
The surface anatomy and features of the head and neck are derived from skeletal and soft tissue structures covered by skin and connective tissue that covers the underlying bony skull. In some areas, particularly the face, the skin is thin, allowing easy palpation of underlying skeletal features. It is also highly mobile as a result of the presence of a number of small but extensive subcutaneous muscles of facial expression, all supplied by a single cranial nerve (facial). The scalp is, in contrast, relatively tough and hidden from view in most individuals by hair. Within the skull, which acts as a protective shield, are the brain and brainstem, with its associated covering of tissue layers and blood vessels. The anatomy is complex and this chapter can only provide an overview of the principal features, with craniofacial anatomy included to link anatomically with the underlying structures, including the neuroanatomy, which may be of particular significance in penetrating or blunt head trauma.
The external face
The anatomical surface features of the face are never totally symmetrical. As facial expressions have evolved as a communication method, the underlying anatomy has evolved from the functional need. The skin is often marked by moles and freckles and may also present with scars consequential to cuts and other trauma.
The shape and size of the hairline vary with race and the eyebrows can also be highly variable.
The nose comprises underlying cartilaginous and bony structures. In the coronal section, the nose is triangular in shape. The external nares (nostrils) are protected by coarse hairs (vibrissae) and serve to filter air entering the nose. The anterior part of the nose is composed of flexible underlying fibrocartilage.
Inferior to the nose is the mouth, surrounded by the lips. Here, the size and shape of the mouth are very variable, both within races and between different racial groups. The lips have non-keratinised epithelium and thus appear pink as a result of the underlying blood vessels.
The eyes are set within the bony orbits of the skull but protected by the rim of bone. Their individual position relative to the nose is variable and can be close-set or wide set in normal individuals. Attached within the orbits are the muscles that control eye movement while, superficially, the paired eyelids cover and protect the eye from potential damage. The lids normally permit only a portion of white sclera to appear laterally, with the transparent conjunctiva and cornea that cover the pigmented iris seen medially. The upper lid normally overlaps the iris, but the sclera may be seen between the iris and the lower lid. The shape of the lids can vary between individuals; in particular, the elevator of the upper lid can be weak or damaged, leading to a drooping appearance.
Ethnic differences are often prominent. Mongoloid epicanthic folds and other minor folds of skin in the medial aspect of the orbit should be noted. Conditions such as exophthalmos associated with hyperthyroidism can result in prominent eyes. Facial fractures affecting the maxilla and inferior margin of the orbit can lead to a sinking of the eyeball. The shape of the lids themselves can lead to a wide range of different appearances of the eye within the orbit.
The internal facial structures
Internally, the muscles of facial expression and their nerve and vascular supplies contribute to the facial structures. In addition, the parotid gland is located within the lateral parts of the cheeks.
The facial expression muscles are supplied by the facial (cranial VII) nerve. Their function is to control and support the structures and openings in the face, such as the eyes and mouth. In humans, their functionality serves an important role in non-verbal communication as well as aiding actions such as screwing up the eyes and chewing. The mouth is surrounded by the sphincteric orbicularis oris muscle into which merge the fibres of the buccinator, the muscle of the cheek. The buccinator contracts during chewing and serves to prevent trapping of food within the space between the gums and teeth; it also acts to raise the pressure of air expelled by musicians playing wind instruments or by whistling. The orbicularis oculi surrounds the eye and serves to function in two ways. First, fibres that surround the eye serve to screw the eye up because they are attached to the bone on the medial aspect of the orbit. Second, the palpebral fibres attach to the lateral palpebral raphe and serve to close the eye when blinking. Additional fibres are attached to the lacrimal sac and serve to dilate the sac and keep the puncta in contact with the eyeball.
The facial nerve enters the face by passing through the tough fibrous capsule of the parotid gland and can be damaged during surgical procedures to that gland.
The nose
The nose, as the upper part of the respiratory tract, is located superior to the hard palate and contains the organ of smell. It is divided into right and left nasal cavities by the nasal septum, with each nasal cavity having an olfactory and a respiratory area.
The external nose varies considerably in size and shape in individuals and races because of differences in the nasal cartilage structure. The inferior aspect is composed of two openings called the nares (nostrils), each separated from the other by the nasal septum. The nasal bones, the frontal processes of the maxillae, the nasal part of the frontal bone and the bony part of the nasal septum form the skeletal components of the nose, whereas five main cartilages form the cartilaginous nose. These are two lateral cartilages, two alar cartilages and a septal cartilage that articulates with the bony septum.
The nasal cavities open through the choanae into the nasopharynx at the posterior. The nasal mucosa is bound closely to the periosteum and perichondrium of the nasal bones and cartilages, and lines the nasal cavities, except for the vestibule which is lined with skin. The olfactory area lies superior within the cavity and is the organ of smell, with its nerve fibres passing through the cribriform plate to enter the olfactory bulbs, which lie against the inferior surface of the frontal lobe of the brain.
The narrow, curved roof of the nasal cavity is divided into frontonasal, ethmoidal and sphenoidal parts, named by adjacent bones. The wide floor is formed by the horizontal plate of the palatine bone and the palatine process of the maxilla. Medially, the wall is the nasal septum, comprising the vomer, perpendicular plate of the ethmoid, septal cartilage and the nasal crests of the maxillary and palatine bones. The lateral walls of the nasal cavity are made up of three nasal conchae or scroll bones, each forming a roof over a meatus connecting the nasal cavity to a sinus or the orbit. The superior meatus is between the superior and middle conchae, into which orifices from the posterior ethmoidal sinuses open. The middle meatus, inferior to the middle conchae, communicates with the frontal sinus via the frontonasal duct and the maxillary sinus at its posterior end. The inferior meatus is inferolateral to the inferior conchae and receives the nasolacrimal duct from the lacrimal sac into its anterior portion.
The nose receives arterial blood from many branches, including the sphenopalatine artery, ethmoidal arteries and the facial artery. Kiesselbach's area, found on the anterior nasal septum, is rich in capillaries and is the site of profuse nose bleeding. The nerve supply of the nasal mucosa is by the maxillary nerve, nasal branches of the greater palatine nerve and the anterior ethmoidal nerves, and branches of the nasociliary nerve.
The paranasal sinuses are air-filled extensions of the nasal cavity within the frontal, maxillary, sphenoid and ethmoid bones and are named according to each bone. The ethmoidal sinuses consist of ethmoidal cells located within the ethmoid bone between the orbit and nose. The sphenoid air sinuses are unevenly divided like the frontal air sinuses and separated by a bony septum. They occupy the body of the sphenoid bone and are separated by thin bone from the optic chiasma, the pituitary gland, the internal carotid arteries and the cavernous sinuses.
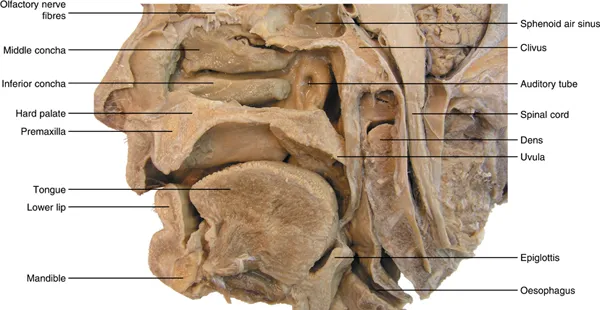
The maxillary sinuses are large pyramidal cavities within the maxillae. Their floor is formed by the alveolar part of the maxilla, with the roots of the maxillary teeth, particularly the first two molars, creating conical elevations (Figure 1.1).
Figure 1.1 The nasal cavity and associated structures.
The oral cavity
The oral cavity consists of the oral vestibule and the oral cavity. The vestibule is the space between the lips and cheeks and the teeth and gums, and communicates with the exterior through the orifice of mouth, the size of which is controlled by muscles, including the orbicularis oris.
The oral cavity lies posterior and medial to the upper and lower dental arches and is limited posteriorly by the terminal groove of the tongue and palatoglossal arches and anteriorly and laterally by the maxillary and mandibular arches containing the teeth. The roof is formed by the hard and soft palate, which also forms the floor of the nasal cavities. Posteriorly, the oral cavity communicates with the oropharynx. If the mouth is closed, the tongue fills the space of the oral cavity.
The hard palate forms the anterior component of the roof of the oral cavity, with its cavity filled by the resting tongue when it is at rest and formed by the palatine processes of the maxillae and the horizontal plates of the palatine bones. The incisive fossa and the greater and lesser palatine foramina open on the oral aspect of the hard palate.
The soft palate is the muscular posterior part, attached to the posterior border of the hard palate and extending as a posteroinferiorly curved free margin that terminates in the uvula. It is strengthened by a palatine aponeurosis formed by the expanded tendon of the tensor veli palatini and is attached to the posterior margin of the hard palate. Laterally, it is continuous with the wall of the pharynx and joined to the pharynx and tongue by the palatopharyngeal and palatoglossal arches. The masses of lymphoid tissue forming the palatine tonsil lie within the tonsillar fossa, bounded by the palatoglossal and palatopharyngeal arches and the tongue.
The orbit
The orbit is a pyramidal, bony cavity in the face. It contains and protects the eye with its associated muscles, nerves and vessels and the lacrimal apparatus. The roof is formed by the orbital part of the frontal bone, separating the orbit from the anterior cranial fossa and containing a small fossa for the lacrimal gland. The lesser wing of the sphenoid contributes to the roof at its apex. The medial wall is formed by the thin bone of the ethmoid, frontal, lacrimal and sphenoid bones. It is indented by the fossa of the lacrimal sac and nasolacrimal duct. The lateral wall comprises the frontal process of the zygomatic bone and the greater wing of the sphenoid, and is vulnerable to direct trauma. It serves to separate the orbit from the tem...
Table of contents
Cover
Half Title
Title Page
Copyright Page
Contents
Preface
Contributors
1 Anatomy of the head and neck
2 Clinical aspects of head injury
3 Imaging of head trauma
4 Biomechanics of primary traumatic head injury
5 Techniques
6 Scalp, facial and gunshot injuries
7 Adult skull fractures
8 Intracranial haematomas – Extradural and subdural
9 Subarachnoid haemorrhage and cerebrovascular traumatic pathology
10 Contusional brain injury and intracerebral haemorrhage – Traumatic and non-traumatic
11 Traumatic axonal injury
12 Brain swelling, raised intracranial pressure and hypoxia-related brain injury
13 Sudden unexpected death in epilepsy
14 Contact sport and blast-related neuropathology
15 Head injury in the child
16 Spinal injuries
17 Difficult areas in forensic neuropathology: Homicide, suicide or accident
18 Non-traumatic neurological conditions in medico-legal work
19 Alcohol, drugs, toxins and post-mortem toxicology
20 The role of the expert witness
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Forensic Neuropathology by Helen Whitwell, Christopher Milroy, Daniel du Plessis, Helen Whitwell,Christopher Milroy,Daniel du Plessis in PDF and/or ePUB format, as well as other popular books in Medicine & Forensic Medicine. We have over 1.5 million books available in our catalogue for you to explore.