eBook - ePub
Atlas of Imaging of the Paranasal Sinuses, Second Edition
- 288 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Atlas of Imaging of the Paranasal Sinuses, Second Edition
About this book
With color illustrations, the Second Edition of this best-selling guide concentrates on the advances in technology that are now available to the clinical otolaryngologist. This reinforces the book's position as a classic guide, especially to the problems associated with endoscopic sinus surgery.
Information
6 Anatomical variants of the ostiomeatal complex in the paranasal sinuses
DOI: 10.1201/9781003076438-6
Messerklinger demonstrated that ventilation and drainage of the anterior ethmoid sinus, the maxillary sinus, and the frontal sinus are dependent upon the patency of the ostiomeatal complex through which these sinuses connect into the nasal cavity.
Most sinus infections are rhinogenic in origin and spread from the ostiomeatal complex to secondarily involve the frontal and maxillary sinuses. The small clefts of the ostiomeatal complex in the lateral nasal wall are easily narrowed or occluded by mucosal edema, resulting in impaired ventilation, failure of mucociliary clearance, and the stagnation of mucus and/or pus in the larger paranasal sinuses.
This process is usually reversible, and once the ostiomeatal complex is reopened, the secondary disease within the larger maxillary and frontal sinuses usually resolves spontaneously. If, however, there is an anatomical variant that narrows these key ethmoid clefts, then a minimal amount of mucosal edema may predispose the patient to recurrent infections and may result in chronic inflammatory changes in the mucosa.
Previously, surgical procedures to alleviate recurrent or chronic inflammatory episodes have been directed at the larger paranasal sinuses. The ventilation of these sinuses was improved by creating new and theoretically effective alternative drainage pathways. The alternative drainage procedures, such as an inferior meatal antrostomy, are now known not to redirect the flow of mucus through the newly created opening (antrostomy), but only to act as ‘drains’ when the mucociliary system is overwhelmed by mucus and pus. The persistence of symptoms following these procedures is usually secondary to persistent disease in the anterior ethmoid affecting the natural ostia and the ostiomeatal complex. When ostiomeatal complex disease is present, recurrent sinus infections may also occur despite there being a widely patent natural accessory ostium.
Functional endoscopic sinus surgery is directed at the natural drainage pathways. The limited surgical resection of tissue that widens these natural clefts and improves sinus ventilation usually leads to a reversal of the mucosal disease in the larger paranasal sinuses. Direct endoscopic examination and visualization of the small clefts of the ostiomeatal complex are not possible, and consequently computed tomography (CT), especially in the coronal plane, is essential for the assessment of the patient with recurrent or persistent sinusitis. Coronal CT allows the radiologist to determine the site and extent of disease in the paranasal sinuses and in the surrounding soft tissues and to identify those anatomical variants that may predispose the individual to sinusitis. Although it is recognized that anatomical variations occur in individuals with no history of rhinosinusitis, variations of the size or position of the normal structures in the lateral nasal wall can impede optimal sinus drainage and occur alongside recurrent sinusitis. Important anatomical variants in the sinuses and the nasal cavity of which surgeons must be aware prior to any intervention are discussed in this chapter.
These important anatomical variants are listed in Table 6.1.
|
AGGER NASI CELLS (Figures 6.1–6.5)
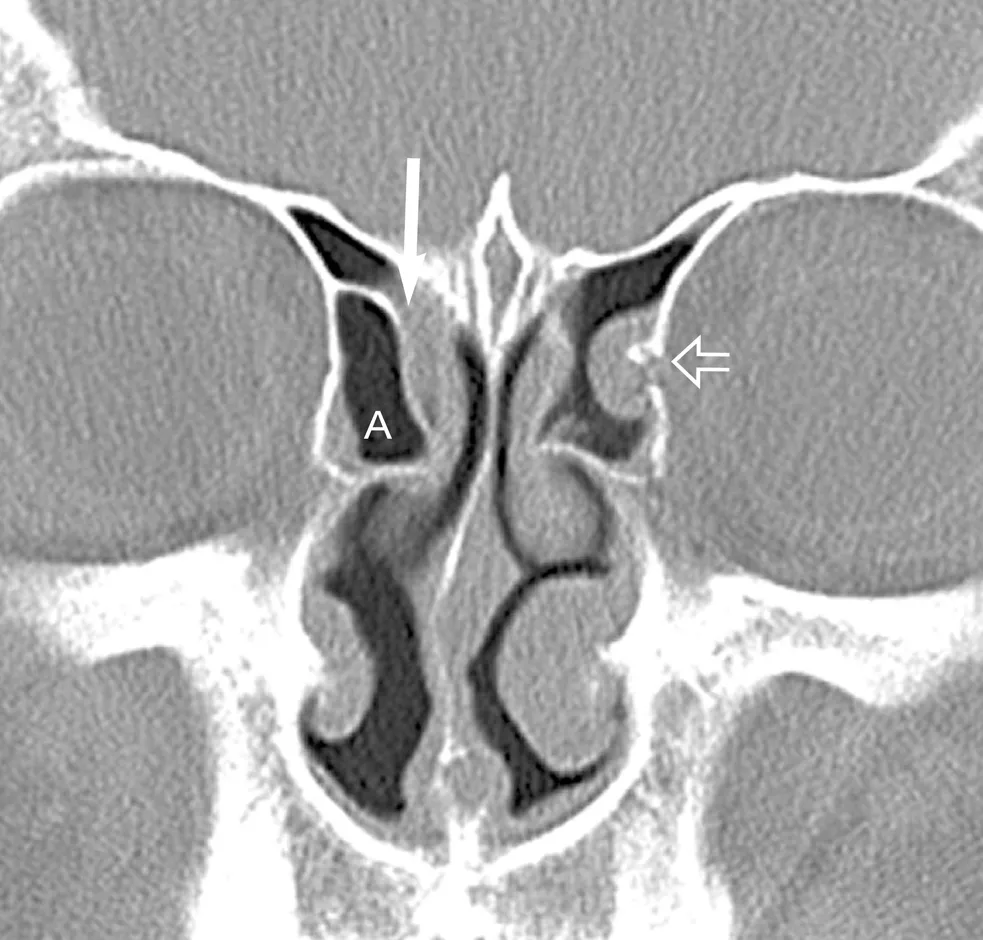
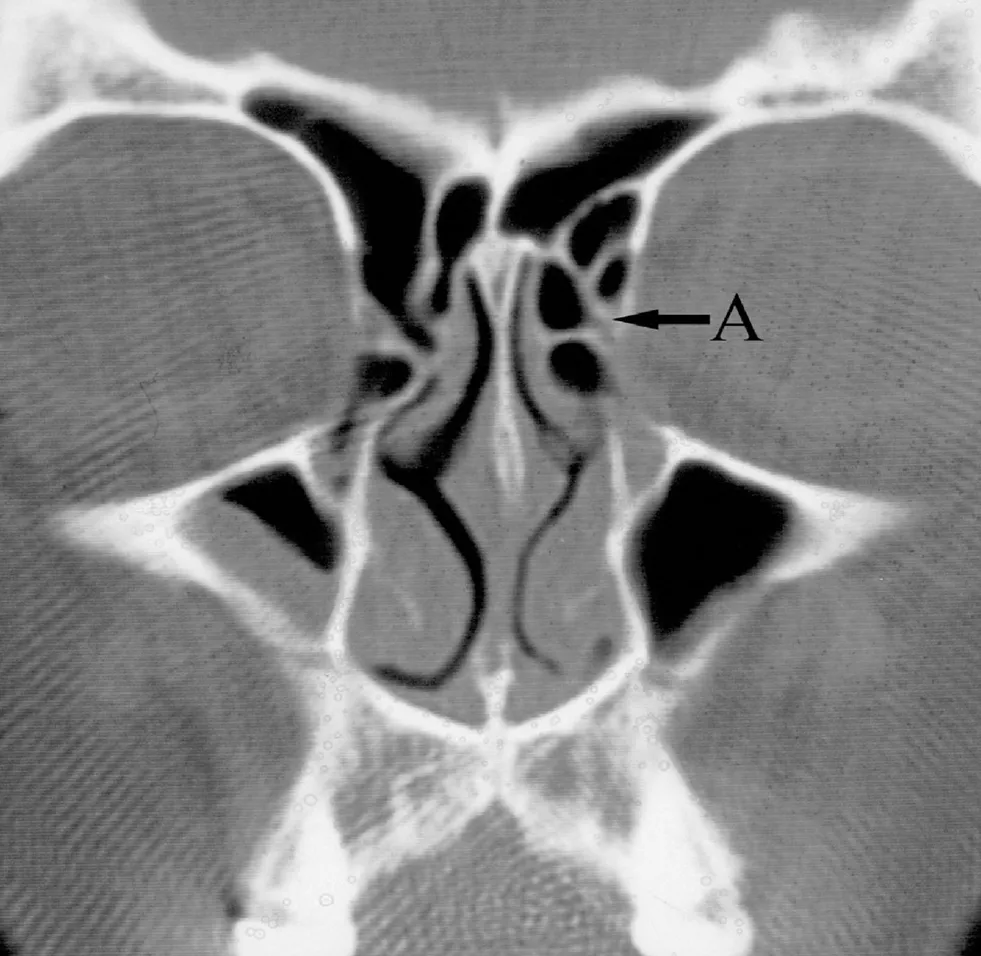



Table of contents
- Cover Page
- Half-Title Page
- Title Page
- Copyright Page
- Table of Contents
- Contributors
- Acknowledgments
- Introduction
- Nasal physiology
- Gross and sectional anatomy of the nasal cavity and paranasal sinuses
- Computed tomography of the paranasal sinuses
- The normal anatomy of the paranasal sinuses as seen with computed tomography and magnetic resonance imaging
- Anatomical variants of the ostiomeatal complex in the paranasal sinuses
- The radiological features of benign inflammatory paranasal sinus diseases
- Complications of sinusitis
- Tumors and tumor-like conditions of the sinonasal cavity
- The postoperative appearances of the paranasal sinuses
- Congenital facial and paranasal sinus abnormalities
- Imaging of midface and paranasal sinus trauma
- Bibliography
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Atlas of Imaging of the Paranasal Sinuses, Second Edition by Lalitha Shankar, Kathryn Evans, Lalitha Shankar,Kathryn Evans in PDF and/or ePUB format, as well as other popular books in Medicine & Diagnostics Imaging. We have over 1.5 million books available in our catalogue for you to explore.