- 912 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Radiology of the Chest and Related Conditions
About this book
The book presents a comprehensive overview of the various disease processes affecting the chest and related abnormalities. It discusses biopsy and bronchography, as well as a variety of imaging techniques including radiography, fluoroscopy, tomography, and ultrasound.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
Pulmonary & Thoracic MedicineChapter 1: Reading of Chest Radiographs Some basic Anatomy and Physiology; including Pleural Fissures, Mediastinal Lines, The Bronchi and Para-Tracheal Lines, Hilar Anatomy, the Pulmonary Lobules, Acini and Lung Cortex, Distribution of Lung Disease in Relation to Anatomy and Physiology, Basic CT and Pathological Anatomy.
DOI: 10.4324/9780429272967-1
Reading of chest radiographs.
In reading chest radiographs it is important to understand their limitations, basic anatomy and some physiology, and to have a systematic system of scrutiny. In this chapter the author goes into most of the points in some detail, as they have a profound influence on what can be seen. High KV (or similar digital) views are considered as essential by the author as the standard for most purposes, as many low KV examinations can fail to display 30% or more of the lungs, particularly the retrocardiac, and retro-diaphragmatic areas and areas hidden by the ribs.
Value of high KV technique - It is essential to have a good technique for chest radiography, as abnormalities which should be noted may otherwise be missed. In many centres chest radiographs are still taken even now with low or inadequate KV (e.g. 50 to 70), and with a 6 ft (approx. 2 metre) focus-film distance (f.f.d.). Such techniques may easily miss or inadequately demonstrate lesions in the lungs, fail to show the larger air passages and may completely miss gross mediastinal abnormalities, such as enlarged nodes, etc. Quite often the descending aorta and the various mediastinal lines are invisible within the 'white area' covered by the heart, or the domes of the diaphragm. The subcarinal area is not displayed, and masses or nodal enlargements here may be entirely missed - this probably accounts for the usual text-book statement that nodal enlargement in sarcoidosis is typically hilar, whereas the largest nodes are often in the subcarinal and azygos regions (see also p. 19.67).
Mediastinal visibility is an essential part of chest radiography, since it is only by noting the presence, displacement or absence of the normal lines, that many abnormalities will be detected. Loss of a mediastinal line or organ outline will usually indicate adjacent disease (see 'loss of silhouette sign' - p. 2.25). Air may often be seen in the oesophagus, and may be a good indicator of normality, dilatation or displacement. Two references emphasise these points:
Evans et al. (1968): Only about 25% of the lungs are unobscured on most conventional chest radiographs. Chotas and Ravin (1995): 26.4 % of lung volumes and 43 % of lung areas are obscured by the heart, mediastinum and diaphragm on many frontal chest radiographs.
Viewers used to studying fairly contrasty low KV radiographs may have some initial difficulty in interpretation of high KV or digital radiographs, but will usually soon prefer the latter (and especially digital high KV radiographs) that contain so much more information.
Because calcification may be less readily seen, a low KV radiograph may be taken as well in a few cases (Illus. HIGH & LOW KV). However for the initial detection of disease or anatomical abnormality, the high KV has so many advantages that the author is greatly surprised that it is not universally used in the UK, despite the slightly increased initial cost of such an installation. It seems quite wrong to regard as the standard chest radiograph, one which displays only about two-thirds of the lungs, and almost totally neglects the mediastinum and the larger air passages.
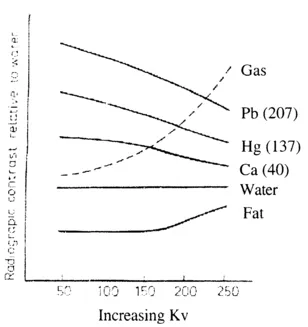
Fig. 1.1 Graph showing relationship between radiographic contrast and increasing KV for the various contrast agents and the body tissues. Numbers in brackets refer to atomic weights.
The high KV and digital techniques are further considered in Chapter 20.
| 1. Soft tissue abnormality - breasts (absence, gynaecomastia, etc.). |
| 2. Symmetry of two sides of the chest (a) lung disease. |
| (b) skeletal. |
| 3. Real or apparent increased translucency. |
| 4. Symmetry in number of blood vessels in either lung: |
| - a 50 % loss in one (or both) = loss of expansion of a major lobe, |
| - note loss of upper or lower lobe vessels (note deviation from normal pattern). |
| 5. Alteration in size of vessels |
| (a) bilateral - congestion |
| plethora (e.g. with intra-cardiac shunt) |
| oligaemia |
| (b) unilateral - Swyer James/Macleod syndrome |
| Oeser sign (spasm from hypoxia due to endobronchial obstruction). |
| (c) proximal dilatation with peripheral pruning - |
| pulmonary hypertension |
| pulmonary embolism. |
| 6. Position, patency or distortion of the trachea, carina and larger bronchi. |
| 7. Diminished volume of a lung or lobe, altered position of fissures, bronchi or pulmonary vessels. |
| 8. Obstructive emphysema (especially on expiration views). |
| 9. Intra-pulmonary consolidation, masses, nodules or other shadows, e.g. septal line engorgement, fibrosis, etc. |
| 10. Loss of part of the cardiac, aortic, SVC or diaphragmatic outline - ‘loss of outline’ or ‘loss of silhouette sign’ - see p.2.25. |
| 11. Pleural abnormality - fluid, air, thickening, mass, etc. |
| 12a. Diaphragmatic elevation caused by: - phrenic nerve palsy, eventration, secondary to lung collapse or hepatic enlargement, or mimicked by fluid or trans-diaphragmatic hernia. |
| 12b. Diaphragmatic depression caused by lung distension. |
| Note that the right side is more commonly higher than the left (see also p. 15.6). |
| 13. Presence of mediastinal and/or hilar masses - nodes, other tumours or cysts, dilated aorta, oesophagus, hiatal hernia, etc. - always study the mediastinal lines. |
| 14. Bone lesions - ribs, spine, sternum, scapulae, etc. |
| 15. Other abnormalities of the chest wall. |
| 16. Position or absence of fundal gas bubble, size of liver, site of gas in the transverse colon, etc. |
Comment: It seems a great pity that many clinicians and radiologists as well, do not really look for the signs of incomplete chest expansion (reduced volume and vessel changes), when a visual inspection of chest movement and its expansion is one of the first observations that is made in every clinical examination of the chest. This lack of appreciation of the findings in partial collapse, together with low radiographs, and the poor demonstration of the mediastinum, has been a major problem in chest radiography. CT (particularly HRCT) has greatly helped in the investigation of the mediastinum and with diffuse lung disease.
On Lateral Views (details on ps. 1.26 to 1.32).
- Similar points as on frontal views i.e. soft tissue abnormalities, symmetry, altered position of fissures, pleural fluid, visible lung (or lobe) outline indicating a pneumothorax, presence of lung, hilar or mediastinal masses, consolidation, signs of congestion, loss of silhouette - heart, diaphragm etc., elevated or 'humped' hemidiaphragm, abnormalities of visceral gas shadows, bony abnormalities, etc.
- Particular attention to:
- (i) Tracheal gas column, and stripes, carina, ring shadows of main bronchi.
- (ii) Vascular patterns in the two lungs, especially the pulmonary arteries, which have different patterns on each side (Figs. 1.33 - 1.35 and Chapter 7).
- (iii) The normally transradiant upper anterior mediastinum above the heart.
- (iv) The normally transradiant retrocardiac area.
- (v) The subcarinal area.
- (vi) Differences between the two lungs - volume, partial collapse, or over-expansion, absence of normal vascular shadows, etc.
Pleural fissures.
Oblique (or major) and horizontal (minor or lesser) fissures
The normal position of these is well known. The oblique fissures normally run from about the level of the D6 vertebral body posteriorly to the anterior costophrenic angles at about the level of the ninth costo-chondral-junction, with the left slightly more vertical and posterior in its lower part (Fig. 1.4 ). This difference in orientation is probably related to the presence of the heart on the left.
The oblique fissures do not run completely in the same plane and are somewhat obliquely orientated and undulating. Below the lower lobe bronchial levels, the central (and lateral, on the left) parts of each oblique fiss...
Table of contents
- Cover
- Half Title
- Title
- Copyright
- Table of Contents
- Preface and Introduction.
- Collection information re main picture collection - (also included in Image AXS Collection Information on CD-ROM).
- Chapter 1: Reading of Chest Radiographs, Some basic Anatomy and Physiology including, Pleural Fissures, Mediastinal Lines, The Bronchi and Para-Tracheal Lines, Hilar Anatomy, The Pulmonary Lobules, Acini and Lung Cortex, Distribution of Lung Disease in Relation to Anatomy and Physiology, Basic CT & Pathological Anatomy, Some Notes re Terminology.
- 2: Lung Consolidation, Ground Glass Shadowing, Obstructive Emphysema, Collateral Air-drift, Mucocoeles, patterns of Collapse, Lung Torsion and Herniation.
- 3: Tracheal and Bronchial Developmental Abnormalities, and Inflammatory Diseases including Bronchiectasis, Cystic Fibrosis and Bronchiolitis.
- 4: Lung and Tracheo-Bronchial Tumours - main types. (a) Historical Review and some General points, (b) Peripheral Tumours, infection complicating tumours, (c) Central Bronchial Tumours, (d) Tracheal Tumours, Papillomas and Endobronchial Deposits.
- 5: Less Common Lung and Bronchial Tumours; Bronchiolo-Alveolar Ca., Carcinoids, Hamartomas, Reticuloses, Protein Disorders, Lung Deposits and Leukaemia.
- 6: Cavitation, Thin-walled Cysts and Bullae, their Association with Tumours. Emphysema. Fat and Calcification. Spurious Tumours. Intravascular, Pulmonary Interstitial & Mediastinal Gas, and Pneumoperitoneum.
- 7: The Pulmonary and Bronchial Vessels, Pulmonary Vascular Abnormalities including Embolism, Pulmonary and Bronchial Angiography, and A/V Malformations.
- 8: Pulmonary Oedema, Lymphangitis Carcinomatosa and ARDS.
- 9: Systemic Veins of the Thorax.
- 10: The Aorta and Related Disorders (except trauma).
- 11: Chest Trauma, Iatrogenic Trauma including drainage tubes and some Post-surgical Conditions and Complications of Radiotherapy.
- 12: The Neck, Thoracic Inlet and Outlet, the Axillae and Chest Wall, the Ribs, Sternum and Clavicles.
- 13: The Thoracic Lymphatic System and Lymph Nodes, and the Spread of Tumours within the Lungs, the Tracheobronchial Tree and the Mediastinum.
- 14: The Extra-Pleural and Pleural Spaces, including Plombages, Pleural Tumours and the Effects of Asbestos.
- 15: The Phrenic Nerves, Diaphragm and Pericardium.
- 16: The Oesophagus.
- 17: The Spread of Chest Tumours to the Abdomen, and some Abdominal Tumours to the Chest - also a consideration of some relevant abdominal conditions in differential diagnosis, particularly of the Liver, Spleen and Pancreas.
- 18: The Mediastinum (including pre-and para-spinal lines, neural tumours, and pneumomediastinum).
- 19: Inflammatory, Hypersensitivity and Immune Lung Diseases, including Parasitic Diseases.
- 20: Techniques for Chest Radiography, Fluoroscopy, Tomography (including CT and MR) and Ultrasound.
- 21: Biopsy etc. Procedures and Bronchography.
- 22: Skeletal, Muscle, Brain, etc. Deposits and some Isotope Procedures.
- 23: Hormonal and Para-Neoplastic Syndromes - also Skin Lesions.
- 24: Lung Cancer (a) Diagnosis and Causes, Smoking Habits, etc. (b) Types of Lung Cancer, Clinical and Radiological Features of the Different Types. Cell types in the lungs, (c) The Radiologists' Role in the Investigation of Lung Cancer. TNM Staging, and the value of Radiological Surveys of Screening for the Detection of Lung Cancer, (d) Patient Management - Possible Treatment Regimes and their Effects. Possible surgery.
- Appendices 1. Radiation Dosage from Chest Radiography and Tomography, including CT
- 2. Threshold Visibility of Pulmonary Shadows on Radiographs, and Perceptual Problems in their Recognition
- 3. Mach Bands
- 4. Some Royal Chest and Smoking Related Illnesses
- Subject Index to Text pages.
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Radiology of the Chest and Related Conditions by F W Wright in PDF and/or ePUB format, as well as other popular books in Medicine & Pulmonary & Thoracic Medicine. We have over 1.5 million books available in our catalogue for you to explore.