Originally published in 1982, this volume deals with behavioral medicine and clinical psychology. Much of what psychologists had been able to contribute to the study and treatment of health and illness had, to this point, been derived from clinical research and behavioral treatment. This volume presents some of this work, providing a fairly comprehensive view of the overlap between behavioral medicine and clinical psychology. Its purpose was to present some of the traditional areas of research and practice in clinical psychology that had directly and indirectly contributed to the development of behavioral medicine. Before the 'birth' of behavioral medicine, which subsequently attracted psychologists from many different areas ranging from social psychology to operant conditioning, the chief link between psychology and medicine consisted of the relationship, albeit sometimes fragile and tumultuous, between clinical psychology and psychiatry. Many of the behavioral assessment and treatment methods now being employed in the field of behavioral medicine were originally developed in the discipline of clinical psychology.
eBook - ePub
Handbook of Psychology and Health, Volume I
Clinical Psychology and Behavioral Medicine: Overlapping Disciplines
- 550 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Handbook of Psychology and Health, Volume I
Clinical Psychology and Behavioral Medicine: Overlapping Disciplines
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
1
Neuropsychological Assessment
DOI: 10.4324/9781003161530-1
NEUROPSYCHOLOGY
Preface
In recent years there has been a rapid and evident increase in activity of psychologists in the areas of internal medicine, surgery and preventive or community medicine. This practice is termed behavioral medicine or medical psychology and the publication of books and journals with these terms in the title testifies to a spread of interest (e.g. Davidson & Davidson, 1980, Norton, 1982, Rachman, 1977). With regard to two of the medical specialties, however, collaboration with psychology has a longer history. The first of these, of course, is psychiatry with which clinical psychology has been identified virtually since the latter’s inception. The other is neurology. Beginning as a part of clinical psychology, then taking on an identity of its own, neuropsychology has a history extending at least as far back as the First World War and represents the first major category of psychological practice addressed to non-psychiatric patients. It might thus be seen as the forerunner of contemporary medical psychology.
In the first section of this chapter we review briefly the history of brain-behavior relationships particularly with regard to the issue of localization. The second section summarizes some of the findings in disease of the various lobes of the cerebral hemispheres. These findings emerge from diverse sources including clinical neurology, experimental psychology, and clinical neuropsychology. Clinical diagnostic methods of neuropsychology are described in the third section which includes case examples from the writer’s experience. This section also briefly discusses treatment approaches to the remediation of the behavioral con-sequences of brain disease. It is hoped that the chapter will give the reader a sense of from whence neuropsychology has come and an appreciation of its current status within the general framework of relations between psychology and medicine.
HISTORICAL INTRODUCTION
Psychology and Neurology
Neurology is the medical specialty concerned with the disease of the nervous system which includes the brain. It has been known, or at least suspected, for a very long time that the brain plays a special role in relation to behavior and experience. The ancient Egyptians thought this was the case as did Hippocrates and Galen, and, in fact, the simple expedient of bashing someone on the head and observing that, if he survives, he acts funny might have convinced primitive man that the head and its contents have more to do with the way people act than do, say, the toes. The empirical observation, however, as is usual with empirical observations, raises more questions than it answers and the process of answering those questions has preoccupied physicians and philosophers for centuries. The questions have to do with mechanism, with specifying the nature of the relationship between brain and behavior. Neurologists, since they treat people with disease of the brain, have found themselves in an especially advantageous position vis a vis these questions, and neuropsychologists, by virtue of their relationship to neurologists, find themselves similarity advantaged.
The whys and wherefores of behavior and experience have been the subject matter of psychology from its beginnings and an interest in the brain as the “organ of the mind,” or more contemporarily, the “organ of behavior,” has always been apparent. This interest has found expression in two subdivisions of psychology: physiological and neuropsychology which differ in a number of respects. The most important difference, I think, lies in the fact that neuro-psychology developed in a clinical, applied context while physiological psychology is a laboratory-based basic science. The strengths and weaknesses of these two ways of doing things have been frequently noted and will not be reiterated here. Suffice it only to note that neuropsychology quite readily became engulfed in neurology because of the shared interest in patients.
Among psychologists, probably no group has adopted the medical model as thoroughly as have neuropsychologists. Certainly many clinicial psychologists working in psychiatric contexts use the medical model of inference to diagnosis from signs and symptoms, yet within clinical psychology there is a strong anti-medical trend engendered, in part at least, by the very serious problems, both conceptual and practical, with psychiatric diagnosis (Blum, 1978; Sandifer, 1972; Ullmann & Krasner, 1975). With the notable exceptions of “organic brain syndrome,” and “minimal brain dysfunction,” neurologic diagnoses do not engender these problems because they are either pathologically based (e.g. tumor) or describe fairly unambiguous symptoms (e.g. seizure disorder). The distinction is not absolute, but there can be little doubt that the pathological, structural bases of neurologic diagnoses are vastly clearer than are those of psychiatric diagnoses, particularly given the inclusion in the Diagnostic and Statistical Manual (DSM III, American Psychiatric Association, 1980) of conditions for which a biological basis is not even suggested. It is not surprising, therefore, that neuropsychologists, somewhat uniquely among psychologists, are comfortable, familiar, and skilled with the application of the medical way of thinking. Certainly if psychology is to impact on the range of medical specialties, an appreciation of the medical model is of some importance and in this regard, neuropsychology might serve as a useful exemplar.
In neuropsychology, the medical model takes the form of diagnostic inference to disease of the brain on the basis of behavioral assessment. Just as the neurologist tries to discover brain disease through the techniques of history taking, physical examination, and laboratory studies, the neuropsychologist tries to discern brain disease through application of his special techniques, usually tests. What psychologists bring to this enterprise is both a technology and a paradigm. Technically, psychometric instruments are among the more sensitive methods available for assessing behavior. They are relatively objective and they yield quantitative data. As regards the paradigm, psychologists think of behavior in ways which neurologists generally do not. That is, as students of behavior, psychologists have developed a variety of taxonomies for behavior which can be brought to bear in trying to understand what is happening to behavior in neurologic disease. There is an important and constant interaction here in that, in neuropsychology, the taxonomy of behavior changes, evolves in light of what happens in neurologic disease. For the psychologist, this process inevitably raises questions about behavior in general, about what neurologic disease might tell us about the structure of behavior in normal circumstances. For example, current thinking in the field of memory has been profoundly influenced by the neuropsychological analysis of amnesic syndromes, yet these very studies rely on methods derived from experimental psychology. Thus, the neuropsychologist brings behavioral expertise to bear in neurology and in the process brings to light phenomena which may have implications for a general theory of behavior.
Brain, Behavior, and the Localization Controversy
The localization issue is an essential part of the question of mechanism, and opinion has waxed and waned over the years from localizationist to wholistic views of brain function and back again. The fundamental question can be simply stated: Are psychological functions geographically arranged in the cerebrum, or rather does the brain act as an undifferentiated whole, at least insofar as “higher functions” are concerned? The question is simple, but the answers have turned out to be complex in the extreme. Let us briefly survey the history of this controversy. By way of preface it is worth mentioning that opinions and speculations about localization historically far out-stripped accumulation of physiological facts, with rather dogmatic pronouncements appearing on the basis of the most meagre sort of data (Esper, 1964). Presently, this circumstance has been largely corrected with contemporary spokesmen tending toward conservatism and one might safely state as a general principle that, the more knowledgeable one is about brain and behavior, the more reluctant he is to make sweeping generalizations about how the two are related.
Bogen (1979) has usefully outlined the major historical positions, breaking them down into five categories. His interest is specifically in views of the corpus callosum, but the model applies to the localization issue more generally. The categories are: humoral theories, traffic theories, classical localization theories, wholistic critical response to classical theories, and two brain or lateralized theories.
The humoral point of view is very ancient and held sway until around the 17th century. The essence of this view which proceeds from the more general humoral theory of disease is that the critical part of the brain from a functional point of view is the ventricular system and the fluid it contains. The brain substance itself was viewed as a supporting structure analogous to the blood vessels in relation to the blood. Specific functions were associated with each of the ventricals, the structure of which had been described, albeit inaccurately, by Galen. This great interest in the ventricals and the cerebrospinal fluid fits the humoral theory of disease, but another possible reason for its preeminence may lie in the fact that dissection of the brain without fixation reveals a structure that is rather undistinguished aside from the fact that it contains huge cavities. Walsh (1978) quotes Sherrington (1951) to this effect.
Vesalius’ famous anatomy text was published in the middle of the 16th century and represented a major advance in knowledge of the structure of the brain. With greater understanding of structure, the idea that the brain substance itself was of major importance grew in prominence and the corollary notion that the connections between structures played a communicative role also arose. Bogen (1979) terms those who favored this view the “traffic anatomists.” Such beliefs rested almost entirely on an anatomical description, however, not physiological experimentation, a circumstance that obtained, in essence, until the 20th century. The rise of faculty psychology coincided with efforts to localize the functions so identified. Gall and Spurzheim’s phrenology was part of this effort and gave rise to the localizationist point of view. Opposing phrenology were a number of writers, perhaps the most prominent among them Flourens. The later wholistic, anti-localizationist points of view claim Flourens a forebearer.
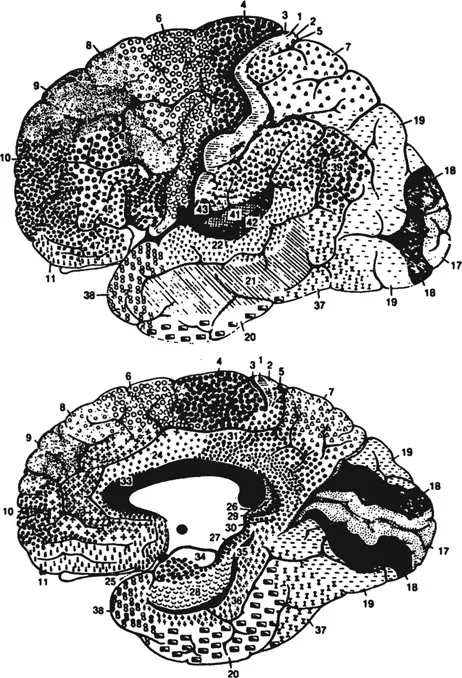
The period of the classical neurologists, beginning toward the end of the 19th century and extending into the 20th, was one of extraordinary creativity, heated debate, and discovery. During this period the issue of localization versus wholismbegan to be addressed on the basis of physiological knowledge and clinical pathologic correlations and the issues raised by these men remain today fundamental issues in clinical neurology and neuropsychology. The period represents one of those unusual confluences which occur episodically in science in which extraordinary men appear on the scene roughly contemporaneously and define the issues for decades to come. Among the names which punctuate this era are: Broca, Wernicke, Liepmann, Dejerine, Pierre Marie, Freud (in his pre-psychoanalytic days), Head, Hughlings Jackson, and the neurohistologists Ramon y Cajal and Brodmann, the latter of whose cortical maps remain the bane of neuroanatomy students to the present day (see Fig. 1.1 and imagine trying to memorize it). The general outlines of the localization controversy can be described. In doing this, Bogen’s fourth category, the critics, will be shown as a reaction to the classical neurologists and the fifth group, the two brain theorists, can be seen to arise out of the clash of these views and in response to more recently emerging data.
Although the lateralization of cerebral control of motor functions had been described by the ancient physicians and demonstrated experimentally by Fritsch and Hitzig, it was Broca’s studies of language impairment whic...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Original Title Page
- Original Copyright Page
- Contents
- Preface
- 1. Neuropsychological Assessment
- 2. Biofeedback: Clinical Applications in Medicine
- 3. Pain: Its Assessment and Management
- 4. Obesity: Etiology, Hazards and Treatment
- 5. Problem Drinking: A Social Learning Perspective
- 6. Changing Smoking Behavior: A Critique
- 7. Sleep Disorders
- 8. Childhood Hyperactivity: Diagnosis, Etiology, Nature and Treatment
- 9. Sexual Dysfunctions
- 10. Psychosomatic Disorders: Basic Issues and Future Research Directions
- 11. Anxiety: Mechanisms and Management
- 12. Affective Disorders
- 13. Lifestyle, Behavioral Health, and Heart Disease
- Author Index
- Subject Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Handbook of Psychology and Health, Volume I by Robert J. Gatchel, Andrew Baum, Jerome E. Singer, Robert J. Gatchel,Andrew Baum,Jerome E. Singer in PDF and/or ePUB format, as well as other popular books in Psychology & History & Theory in Psychology. We have over 1.5 million books available in our catalogue for you to explore.