- 272 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Gynaecology in Primary Care comes at a time of great change in health service delivery. General practice is facing the challenges of developing Clinical Commissioning Groups, providing an ever greater range of primary care services and implementing NICE guidelines, whilst CCGs through their members will be under a legal duty to innovate. From a provider perspective, the book equips general practitioners with up-to-date knowledge of common gynaecological conditions, suggestions of best practice with regard to management and investigations to be undertaken within primary care, and guidelines for onward referral, where this is appropriate and necessary. From a commissioning perspective it provides an invaluable resource to CCGs, to inform their future pathways for gynaecology care. This highly practical book delivers the main aim of the RCP report - to ensure best care for female patients in the setting of their choice and where possible to develop streamlined one-stop services in primary care so that women do not have to take time off from their work and family commitments. It is ideal for general practitioners needing to be inspired and informed, and is also highly recommended for other healthcare professionals and medical students with an interest in women's health. 'Optimal patient care requires many connected features to synchronise effectively. This book describes how this could be achieved by focusing attention on well-crafted, evidencebased clinical pathways. This book advances our thinking on how we connect clinical, system and patient level perspectives on optimal care management.' Denis Gizzi, in his Foreword 'Written by a highly regarded, experienced and practicing GP, who has taken on the role as Clinical Director on behalf of the CCG for this programme area, this book is a valuable asset for both practicing GPs and developing CCGs to ensure that gynaecology services effectively commission, maximise the health of the population, improve the experience of the patient, and improve value for money.' Kath Wynne-Jones, in her Foreword 'An excellent guide to the management of gynaecological problems in primary care for not only clinicians in training, but for more experienced clinicians who look for straightforward and easily accessible advice to support their clinical management decisions. Look no further than this textbook. Dr Sharma's textbook will be a boon to developing organisations in delivering world-class services.' Dr Ian Wilkinson, in his Foreword
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
Medicine1
Dysmenorrhoea
DEFINITION
Dysmenorrhoea is defined as painful menstruation that interferes with a woman’s physical, emotional and social quality of life.1 The term dysmenorrhoea is derived from the Greek words dys meaning difficult/painful, meno, meaning month and rrhea, meaning flow.
Dysmenorrhoea is one of the most common gynaecological problems in young women who present to their general practitioner. Menstrual pain is often described as lower abdominal cramp-like pain, sharp/aching pain that comes and goes, or sometimes back pain during the period. Some pain during periods is normal but excessive pain must not be ignored. Premenstrual symptoms are often present including nausea and vomiting.
It is classified as either primary (spasmodic) or secondary (congestive) dysmenorrhoea.
Primary dysmenorrhoea is defined as recurrent, cramp-like pain occurring during menstruation in the absence of any pelvic pathology. It usually begins in adolescence. Current evidence suggests that primary dysmenorrhoea is due to prostaglandin F2 alpha (PGF2 alpha), a potent myometrial stimulant and vasoconstrictor present in the secretory endometrium.2 This causes an increased myometrial activity resulting in uterine ischemia and pain. The uterine contractions can last many minutes and may produce uterine pressures greater than 60 mmHg. Elevated levels of prostaglandin were found in the endometrial fluid of women with dysmenorrhoea and the level found correlated with the degree of pain.3
Pathophysiology of primary dysmenorrhoea:
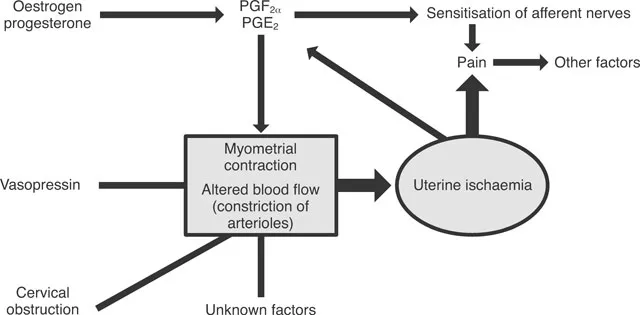
FIGURE 1.1 Pathophysiology of primary dysmenorrhoea
www.sogc.org/guidelines/public/169E-CPG-December2005.pdf
Secondary dysmenorrhoea is defined as menstrual pain resulting from gynaecological pathology, e.g. fibroids, endometriosis or pelvic inflammatory disease.
Prevalence
Dysmenorrhoea is one of the most common gynaecological problems in young women presenting to clinicians.4
Its prevalence is estimated at 25% in women of all age groups. It is most common in adolescents. Ninety per cent of female adolescents tend to suffer with dysmenorrhoea.5 Primary dysmenorrhoea affects up to 50% of postpubertal women.6 Secondary dysmenorrhoea is most common in women aged 30–45 years. Dysmenorrhoea severe enough to cause absence from work occurs in less than 5% of women.7
Risk factors
The following risk factors have been associated with severe episodes of dysmenorrhoea:8
- smoking
- early menarche
- heavy menstrual bleed
- prolonged menstrual bleed
- strong family history
- obesity
- age (symptoms are more pronounced in adolescents than in older women)7
- lower socioeconomic groups4
- frequent lifestyle changes, less social support and stressful relationships.9
Obesity and excess alcohol consumption were found to be associated with dysmenorrhoea in some (but not all) studies.10,11 Physical activity is not thought to be associated with dysmenorrhoea.8 There is some evidence that parous women have less severe dysmenorrhoea.2,10
Primary care management
The optimal management depends on distinguishing between primary and secondary dysmenorrhoea. Although it is not life threatening, it can be debilitating and it is essential that the underlying pathology is identified and treated specifically.
Women suffering from primary dysmenorrhoea do not usually seek medical help and do not make use of available prescription medications. A detailed gynaecological history can easily distinguish between primary and secondary dysmenorrhoea.
History
Menstrual history
Enquire as to the age of menarche, length and duration of bleeding and whether associated with blood clots.
Pain
Enquire about the type, duration, radiation of pain, association with any other symptoms (bladder/bowel), severity and the degree of disability. Ask about all therapies used in the past for pain relief including over-the-counter preparations.
Sexual history
It is important to ask about sexual history, past history of sexually transmitted infections (STIs), vaginal discharge and dyspareunia. Enquire about contraception. Many adolescents use dysmenorrhoea as a pretext to seek contraception.
Family history:
Enquire about any family history of endometriosis. A family history of endometriosis may be an indicator for referral...
Table of contents
- Cover
- Title Page
- Copyright Page
- Table of Contents
- Foreword
- Foreword
- Foreword
- Preface
- About the author
- Acknowledgements
- 1 Dysmenorrhoea
- 2 Premenstrual syndrome
- 3 Menstrual migraine
- 4 Dyspareunia
- 5 Pelvic pain
- 6 Vaginal dryness
- 7 Vulvodynia
- 8 Management of vaginal discharge in primary care
- 9 Pelvic inflammatory disease
- 10 Dysfunctional uterine bleeding
- 11 Postmenopausal bleeding
- 12 Postcoital bleeding
- 13 Intermenstrual bleeding
- 14 Genital prolapse
- 15 Pessary service in NHS Oldham
- 16 Infertility
- 17 Female urinary incontinence
- 18 Urinary retention: a primary care emergency
- 19 Endometriosis
- 20 Menopause
- 21 Understanding gynaecological ultrasound scan
- 22 Polycystic ovary syndrome
- 23 Endometrial cancer
- 24 Uterine fibroids
- 25 Ovarian cancer
- 26 Colposcopy
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Gynaecology in Primary Care by Anita Sharma in PDF and/or ePUB format, as well as other popular books in Medicine & Gynecology, Obstetrics & Midwifery. We have over 1.5 million books available in our catalogue for you to explore.