Acute and chronic liver disease is a global endemic healthcare concern. More than 500 million people around the world are infected with the hepatitis B or C virus. Approximately 500, 000 patients die of hepatocellular carcinoma every year, implying that trained healthcare professionals and facilities for liver disease patients is a critical issue. Although promising therapies have been developed for viral hepatitis infections, management of liver cirrhosis, and hepatocellular carcinoma yet many patients suffer due to lack of adequate healthcare by professional hepatologists. This means that primary care physicians should be informed about diagnosing liver disease and the early management of viral hepatitis and hepatocellular carcinoma. Comprehensive Practical Hepatology provides readers current standard primary care guidelines for treatment and early stage management of patients with liver function abnormalities. This book provides a practical approach for physicians to apply on patients with apparent liver function abnormalities. The guidelines also cover: Acute and chronic liver injury, Information about the liver in systemic diseases, Drug usage in liver diseases, Surgical risk in liver disease patients, and, Recommendations for pregnant as well as elderly patients. Comprehensive Practical Hepatology thus provides complete practical advice on the management of liver diseases to non-hepatologists and general physicians.
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Comprehensive Practical Hepatology
About this book
Trusted by 375,005 students
Access to over 1 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
Gastroenterology & HepatologyApproach to Patients with Chronic Liver Injury
KEY POINTS
- History taking and physical examination are important in the differential diagnosis of chronic liver injury, with history of alcohol or drug taking essential in diagnosing liver disease caused by these materials.
- Type of liver injury should be classified as hepatocellular, cholestatic or mixed, because classification can help narrow the causes of liver injuries and suggest additional and effective history taking or physical examination.
- Symptoms in patients with chronic liver diseases are nonspecific, with the most common being fatigue. Although patients with advanced liver cirrhosis often complain of pruritus, anorexia, leg edema and/or abdominal distension due to ascites retention, most patients with chronic hepatitis and early stage cirrhosis are asymptomatic.
- Differential diagnosis can be a step-by-step process in the absence of severe or advanced liver injury. Elevated T-Bil (>2.0 mg/dl) or elongation of prothrombin time (PT) may suggest severe injury. Although marked elevation of serum aspartate aminotransferase (AST) and/or alanine aminotransferase (ALT) is also an indicator of severe liver injury, there is no clear threshold.
- Frequency of etiologies of chronic liver injury may differ geographically or ethnically, with the order of blood tests based on the prevalence of each disease in that area.
- Primary care providers should be aware of the diagnostic criteria for common chronic liver diseases. These providers should also be familiar with methods used to initially assess liver injury, as well as when to refer patients to specialists.
- Liver biopsy is useful not only to identify etiology, but to determine the grading and staging of liver disease and to assess the likelihood of progression to cirrhosis or liver failure.
- Cirrhosis is often diagnosed by a combination of laboratory data and patient signs and symptoms. In particular, AST/ALT>1, hypergammaglobulinemia and low platelet count (<100,000/μL) support a diagnosis of cirrhosis. Imaging modalities are also helpful diagnostically, and the presence of portal hypertension (suggested by splenomegaly, enlarged portal vein or esophageal varices) strongly supports a diagnosis of cirrhosis.
- Patients with advanced chronic liver diseases are at high risk for the development of hepatocellular carcinoma (HCC), and should be assessed by imaging modalities such as ultrasound (US), CT, and MRI, or by measuring serum concentrations of tumor markers, such as alpha-fetoprotein and des-γ-carboxy prothrombin at regular intervals.
INTRODUCTION
The term “chronic liver injury” usually refers to liver injury lasting longer than 6 months. Practically, however, patients who show mild to moderate abnormalities on liver function tests (LFTs) at two different time points should be suspected of having chronic liver disease. Since second tests have been reported to show resolution of initially elevated levels of bilirubin, AST, ALT, alkaline phosphatase (ALP), and γ-GTP in 12% to 38% of patients, these patients should again be checked after 2-3 months [1]. The frequency of abnormal LFTs in asymptomatic subjects depends on the population studied, and has been found to vary from 0.5% to 8.9%. The causes are shown in Fig. (1).
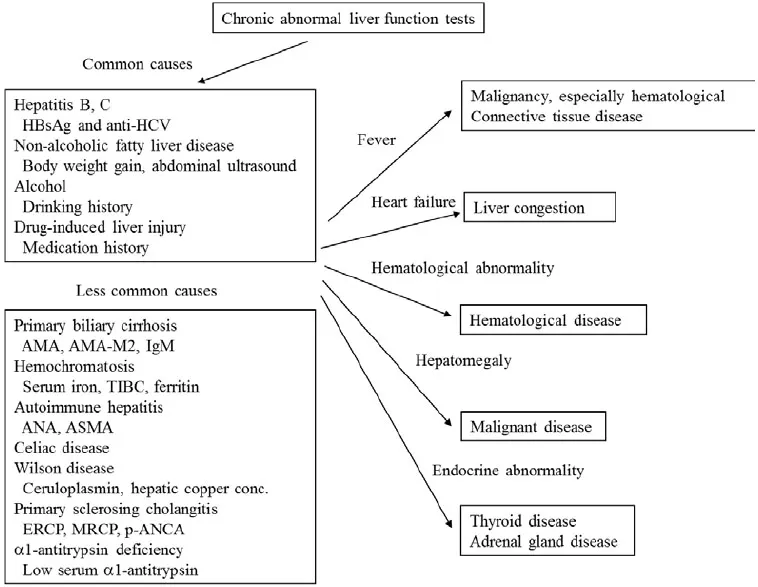
Figure 1)
Disorders causing chronic abnormal liver function tests and their methods of diagnosis. Abbreviations: AMA, anti-mitochondrial antibody; ANA, anti-nuclear antibody; ASMA, anti-smooth muscle antibody; ERCP, endoscopic retrograde cholangiopancreatography; MRCP, magnetic resonance cholangiopancreatography; p-ANCA, anti-neutrophilic cytoplasmic antibody.
HISTORY TAKING
History taking should focus on the following points:
- Use or exposure to medications or chemicals.
An acute form of drug-induced liver injury (DILI) should be particularly suspected in patients who: 1) started taking a new drug within the past 3 months, 2) have a rash, or 3) have symptoms such as fever, general malaise, and skin itching. However, these signs and symptoms may be absent in patients with the chronic form of DILI. Diagnosis may be difficult in some patients because of the long interval between starting a suspected drug and presentation with liver injury.
- Family history of liver disease.
Especially important are family history of hepatitis B and inherited diseases.
- History of hepatitis.
History of acute hepatitis of unknown etiology or after receiving blood transfusion before 1991 may suggest acute hepatitis C, with most of these patients developing chronic hepatitis C. Persistent HBV infection may be present in 5% to 10% of patients with acute hepatitis B, depending on HBV genotype. Of the eight genotypes identified to date, one, genotype A, shows a high rate of chronic hepatitis after acute infection. Patients with resolved acute hepatitis B may have a persistent but low level of HBV replication for a long period of time [2].
- Alcohol consumption.
Alcoholic hepatitis should be suspected in women who consume 30-40 g/day alcohol and men who consume 60-150 g/day. Long term consumption of lower amounts of alcohol can cause alcoholic fatty liver or liver fibrosis.
- History of blood transfusion.
Blood transfusion before 1991 could cause posttransfusion hepatitis.
- History of abdominal operation.
History of jejunoileal bypass surgery may suggest non-alcoholic steatohepatitis (NASH). Operation for gallstones may indicate recurrence of the disease.
7) Presence of autoimmune disease.
Because autoimmune diseases are likely to overlap or occur together, the presence of an autoimmune disease may suggest complication with another autoimmune disease, including autoimmune liver disease.
8) Accompanying symptoms such as fatigue, pruritus, arthralgia, myalgias, rash, anorexia, fever, shaking chills, nausea, and right upper quadrant pain.
Fatigue and pruritus are most often experienced by patients with liver diseases, although neither is specific for liver disease. Liver dysfunction in patients with shaking, chills and fever may be due to bacteremia following biliary tract infection or urinary tract infection. Moreover, many bacterial and viral infections are known to cause abnormal LFT results.
9) Change in body weight.
A recent increase in body weight, usually over 3 kg, suggests nonalcoholic fatty liver disease (NAFLD). Nonalcoholic steatohepatitis (NASH) is also suggested in patients with type 2 diabetes mellitus, hypertension, or hyperlipidemia.
10) Sexual behavior.
Homosexual individuals are at high risk of HIV infection and may be co-infected with HBV.
Use of medications, increased body weight and alcohol consumption, in particular, may often provide clues in identifying causes of liver disease.
PHYSICAL EXAMINATION
Physical examination should focus on the following:
- Jaundice may suggest advanced liver disease or cholestasis.
- Brown skin color may suggest hemochromatosis.
- Skin eruption may suggest drug allergy or cholestasis.
- Xanthelasmata or xanthomata may suggest chronic cholestasis, usually in patients with primary biliary cirrhosis.
- Struma may suggest complicating thyroiditis in patients with autoimmune liver diseases.
- Spider nevi, palmar erythema, gynecomastia, caput medusae, testicular atrophy or muscle wasting may suggest liver cirrhosis.
- Jugular vein dilatation may suggest right-sided heart failure, which could lead to liver congestion.
- Dilated superficial veins of the abdominal wall may represent portal hypertension.
- Hepatomegaly
The size, shape and consistency of the liver should be determined. Most patients with chronic or alcoholic hepatitis show enlarged tender liver palpable below the right costal margin. In contrast, cirrhotic liver can be palpable only around the middle line. A very large liver with consistency may indicate HCC, metastatic liver tumor, or infiltrative liver disease such as amyloidosis.
- Splenomegaly
A palpable spleen usually indicates moderate...
Table of contents
- Welcome
- Table of Contents
- Title
- BENTHAM SCIENCE PUBLISHERS LTD.
- FOREWORD
- PREFACE
- Symptoms and Signs Suggestive of Liver Disease
- Diagnostic Strategies for Patients with Abnormal Liver Function Tests
- Approach to Patients with Acute Liver Injury
- Approach to Patients with Chronic Liver Injury
- Diagnostic Strategies and Treatment of Liver Tumors
- Liver Function Abnormalities in Systemic Disease
- Sytemic Abnormalities in Liver Disease
- Infection and Liver
- Approach to Liver Injury Caused by Drugs and Toxins
- Risk of Surgery and Drug Therapy in Patients with Liver Disease
- Approach to Children with Abnormal Liver Function Tests Results
- Practical Management of Elderly Patients with Liver Injury
- Practical Management of Pregnant Women with Liver Injury
- Lifestyle Recommendation for Patients with Liver Diseases
- Medical Management of Patients Following Liver Transplantation
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Comprehensive Practical Hepatology by Yukihiro Shimizu in PDF and/or ePUB format, as well as other popular books in Medicine & Gastroenterology & Hepatology. We have over one million books available in our catalogue for you to explore.