This second edition continues to present the following special features of its highly successful predecessor:
* an analysis of the major partitionings of the MMPI into special scales in terms of their clinical usefulness, resulting in the selection of those scales that most discriminatingly and non-redundantly represent the core psychological traits and qualities captured by the MMPI;
* a number of individually developed scales that tap into additional aspects of validity, psychopathology, and adjustment and personality;
* the Indiana Special Scales which sample additional areas that were not as well identified or delineated by prior scale development;
* a critique of the foregoing selections in light of the extant MMPI literature (which this second edition further expands up to the current time) and of a major investigation at the Indiana University Medical School of the conjoint use of special scales;
* a critique of the shortcomings of high-point codes;
* a detailed, categorized listing of the most useful scales in empirical clusters based on their established intercorrelations such that not only scale elevations but also interrelations (and the departures from the expected) of scales become clinically interpretable;
* an exploration of the interrelationships between Rorschach and MMPI variables, leading to complementary use of these two instruments.
This second edition also takes into account the development of MMPI-2 and the status of its new special scales vis-a-vis the established scales derived from the original MMPI. In so doing, it indicates why the original scales continue to offer substantial advantages over the MMPI-2 scales. It further examines changes in the nosology of personality disorders and proposes special scale markers for these disorders as they have been clarified progressively through DSM-IV.
This volume offers the MMPI user a library of psychological report statements based on special scale interpretation, with recommended score ranges and cutting points for particular inferences. These latter features appear together as an appendix styled as "The Human Computer." Unlike the typical computer-generated report, this appendix makes all decision rules explicit, thereby permitting the user to use the library of statements with full knowledge of their applicability. By retaining the element of clinical judgment -- the human dimension of inference -- the user is enabled to better integrate MMPI special scale findings with data from other sources while in the process of crafting the report. All of these new features are accompanied by applicable literature citations.
- 200 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
The Clinical Application of MMPI Special Scales
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Subtopic
Mental Health in PsychologyIndex
PsychologyCHAPTER 1
INTRODUCTION
DOI: 10.4324/9781315827421-1
Many verbal inventories for the measurement of psychopathology and personality have been developed over the past 40 years. Some attained modest prominence at least for a time; others were neglected from the beginning and little is known about their attributes and capacities. Only a handful have survived perennially. The outstanding example is the Minnesota Multiphasic Personality Inventory (MMPI). The original MMPI was created 50 years ago but remains the most popular formal assessment tool in psychology and education. It has the deepest potential for evaluating human personality, for measuring change in personal and emotional status, for increasing the accuracy of diagnosis, and for giving useful information regarding treatment plans and prognosis. Thousands of publications, perennial workshops, and computerized interpretive programs testify to the popularity of the MMPI. An estimated 15 million MMPIs are administered in the United States alone each year.
Despite its longevity, the MMPI has a number of methodological defects that have been summarized by Faschingbauer (1979) and Levitt and Duckworth (1984). Wiener and Harmon (1946) observed early that there are two types of statements in the MMPI clinical scales; obvious and subtle. An obvious item is one for which the psychopathological or diagnostic response is clear as, for example, responding “true” to the statement “Life is a strain for me much of the time.” A subtle item is one for which there is no response that is keyed for psychopathology as, for example, “I like Alice in Wonderland by Lewis Carroll.”
Every relevant investigation has shown that the correlations between the obvious and subtle subsections of the clinical scales range from zero to low negative, a certain mathematical argument for dimensional independence. Summing these unrelated subsets into a single score can only be a “cancellation approach” to scale scores (Norman, 1972; Faschingbauer, 1979).
The obvious-subtle differential is not the only criticism that has been leveled at MMPI clinical scales. Faschingbauer (1979) described them as “heterogeneous, redundant, and overlapping … over 100 items are not even scored. How much potentially useful information never enters the code type as a result is still unknown” (p. 374). Faschingbauer is in essential agreement with Norman (1972) who pointed out that the clinical scales are not only “inefficient, redundant, and largely irrelevant for their present purposes” (p. 64) but also the MMPI methods of “combining scale scores and for profile interpretation are unconscionably cumbersome and obtuse” (p. 64). Norman summed up by noting that “it is abundantly clear that they are about as inappropriate and maladapted a set as one could imagine for their current uses in profile analysis, and interpretation and typal class definition” (p. 64). Archer and Krishnamurthy (1993b) theorize that the general absence of correlation between the MMPI and the Rorschach “could be the result of the multidimensional nature of most of the basic MMPI clinical scales” (p. 286).
Wiggins (1966), commenting on the heterogeneity of the clinical scales, remarked that “the hodgepodge of content which contributes to a high score on a given clinical scale is not suggestive of any consistent personality trait or structure” (p. 31). Indeed, the libraries of interpretive statements that have been proposed for high scores on clinical scales are at best unenlightening and at worst, confusing. For example, Graham (1987) listed 44 interpretive statements that can accompany a high score on Scale 4 plus 16 statements that follow from low scores. A high score on Scale 9 yields 42 interpretive statements, a low score, 14 more. Clopton (1979a) pointed out the obvious: Respondents endorsing very different subsets of items can obtain the same raw score on any scale.
Thus, to select the appropriate interpretative statements from among Graham’s lists requires that the clinician examine the protocol’s individual item responses. It is unsafe to make interpretations based solely on the clinical scale score.
To exemplify this phenomenon, Wiggins (1966) created profiles for two hypothetical patients whose clinical scale profiles (see Fig. 1.1) were identical but whose scores on Wiggins’ content scales varied markedly as indicated in Table 1.1.
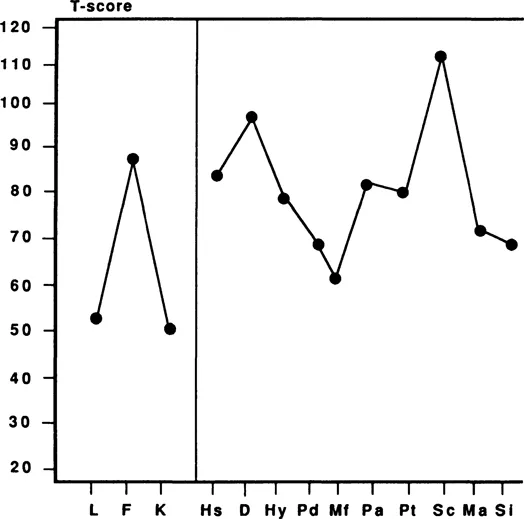
FIG. 1.1. Clinical profile of Wiggins’ hypothetical patients.
| Content scale | Patient A | Patient B | Difference |
|---|---|---|---|
| | |||
| ORG | 28 | 5 | +23 |
| PSY | 8 | 21 | −13 |
| HEA | 7 | 20 | −13 |
| FEM | 6 | 17 | −11 |
| FAM | 11 | 6 | +5 |
| DEP | 15 | 19 | −4 |
| HYP | 8 | 12 | −4 |
| PHO | 13 | 9 | +4 |
| SOC | 10 | 13 | −3 |
| HOS | 9 | 12 | −3 |
| AUT | 13 | 11 | +2 |
| REL | 7 | 9 | −2 |
| MOR | 12 | 11 | +1 |
Obviously, the interpretations of the two identical clinical profiles using high point codes or any other method of analysis would also be identical. Wiggins discussed the differences in interpretation of the two records according to Table 1.1.
Patient A has admitted to a larger number of symptoms thought to be indicative of organic pathology. Additionally, he admits having family problems and a number of psychotic symptoms of a primarily paranoid nature. He is greatly concerned about his health and admits to liking an unusual number of feminine pursuits. By comparison with Patient A, Patient B is generally more deviant with respect to content categories reflecting poor morale, mood instability, social maladjustment and hostility.
The configuration of content scale scores of Patient B readily confirms the impression of psychopathology gained from an inspection of the clinical profile in Figure 1.1. This could be the profile of a paranoid schizophrenic with an underlying homosexual component and a body concern that is delusional in nature. Poor morale, social maladjustment, and hostility are, of course, compatible with this picture.
Although Patient A’s raw content scale scores are sufficiently deviant to be considered those of a hospitalized patient, they are in sharp contrast to those of Patient B. By comparison, Patient A is almost exclusively concerned with organic symptoms and, to a lesser extent, family problems. Evidence of delusional thinking, health concern, feminine interests, and general maladjustment is comparatively weak for Patient A. The clinical scale profile in Figure 1.1 may now be viewed in a quite different light. (Wiggins, 1966, p. 30)
The MMPI clinical scales are not without their defenders. The thrust of the defense is that the clinical scales were intended to measure psychopathology, not personality traits and it is unfair to criticize the MMPI for being unable to do what it has never been intended to do (Dahlstrom, 1969; Butcher & Tellegen, 1978).
Thus, Dahlstrom (1969) pointed out that internal item consistency and homogeneity are not relevant to the task of the MMPI. The important criterion, according to Dahlstrom, is not whether an item correlates with other items but whether it improves clinical prediction about patient groups (i.e., external rather than internal validity).
Dahlstrom added that the obvious and subtle dimensions of clinical scales are relatively uncorrelated among normal persons but have much higher correlations for appropriate psychiatric patient reference groups.
As we see here, the issue of the intent of the MMPI is actually irrelevant but for purposes of completeness of the argument, it might be noted that the original purpose of the MMPI may not be as clearcut as Dahlstrom (1969) and Butcher and Tellegen (1978) suggest. Consider the following quotations from the original MMPI Manual (Hathaway & McKinley, 1951):
The Minnesota Multiphasic Personality Inventory is a psychometric instrument designed ultimately to provide, in a single test, scores on all the more important phases of personality. The point of view determining the importance of a trait in this case is that of the clinical or personnel worker who wished to assay those traits that are commonly characteristic of disabling psychological abnormality … personality characteristics may be assessed on the basis of scores on nine clinical scales originally developed for use with the Inventory … although the scales are named according to the abnormal manifestation of the symptomatic complex, they have all been shown to have meaning within the normal range … as for validity, a high score on a scale has been found to predict positively the corresponding final clinical diagnosis or estimate in more than 60 percent of new psychiatric admissions, (pp. 5–6)
Thus, it appears on the one hand, the constructors of the MMPI are saying that the instrument is intended for differential diagnosis...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Contents
- Preface to the Second Edition
- Special Scales Key
- Chapter 1 - Introduction
- Chapter 2 - The Validity Scales
- Chapter 3 - Some Useful Special Scales
- Chapter 4 - The Assessment of Psychopathology
- Chapter 5 - The Measurement of Adjustment and Personality
- Chapter 6 - MMPI Special Scales and the Rorschach
- Chapter 7 - The Fate of Original MMPI Special Scales in MMPI-2
- Chapter 8 - The MMPI-2 Content Scales
- Appendixes
- References
- Author Index
- Subject Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access The Clinical Application of MMPI Special Scales by Eugene E. Levitt,Edward E. Gotts in PDF and/or ePUB format, as well as other popular books in Psychology & Mental Health in Psychology. We have over 1.5 million books available in our catalogue for you to explore.