![]()
01
Chapter 1
Rheumatoid arthritis
Rheumatoid arthritis (RA) is the archetypal autoimmune disease, demonstrating activation of several inflammatory pathways that, without early treatment, results in end-organ damage focused around synovial joints. Since RA is a systemic disease, other organs can also be involved, including the lungs, heart, eyes and central nervous system. The condition has a worldwide prevalence of 1–2%. RA affects women 2–3 times more often than men. Although RA can present at any age, patients most commonly are first affected in the third to sixth decades of life.
In this chapter we discuss the diagnosis, pathophysiology and management of RA in the context of real-life clinical cases. The cases aim to demonstrate the breadth of clinical scenarios in which RA can present, with worked examples of diagnosis and management, particularly in the context of biologic therapies, which have revolutionised RA care worldwide.
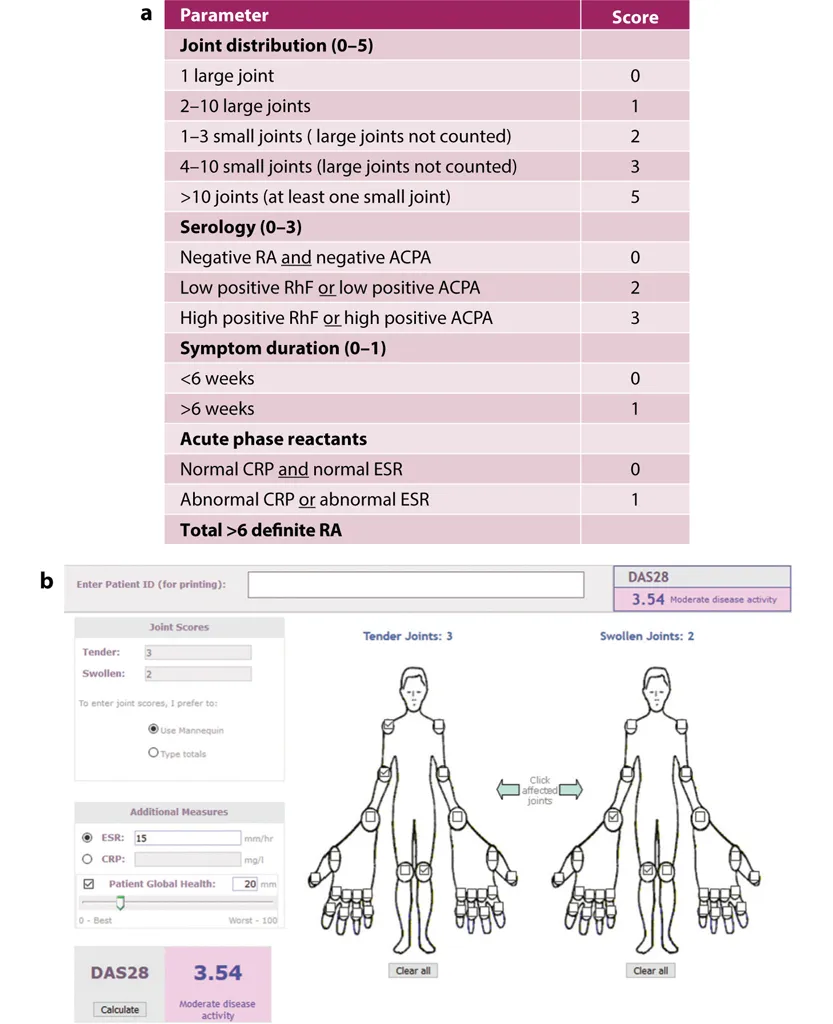
The diagnosis of RA has been aided by the development of classification criteria published in 2010 (EULAR/ACR criteria, see Aletaha et al., 2010). These include features that assist in confirming a diagnosis which is likely to require treatment (summarised in Figure 1.1). The features are based on:
•the pattern of joint involvement (joint distribution scores 0–5)
•the presence of autoantibodies (serology scores 0–3)
•the duration of symptoms, with >6 weeks’ duration of symptoms making the diagnosis more likely (symptom duration scores 0–1)
•the presence of raised inflammatory markers, including erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) (acute phase reactants scores 0–1).
Figure 1.1. EULAR/ACR classification and DAS28 scoring system
(a) EULAR/ACR 2010 classification criteria for rheumatoid arthritis; (b) DAS28 scoring system – a freely available online tool that can be used in the clinic to calculate the Disease Activity Score (DAS) based on 28 joints assessed clinically for swelling and tenderness (see www.4s-dawn.com/DAS28). Scores are entered in the tool, together with inflammatory markers ESR or CRP, with the patient global assessment of their disease on a 0–100mm scale. A numerical DAS28 score is then calculated and recorded.
Depending on the presence/absence of such classification criteria, the criteria define a score. The higher the score, the greater the likelihood of confirming RA which is likely to require treatment intervention to achieve symptom control; a score >6 means a definite diagnosis of RA.
Prominent features of RA in comparison to osteoarthritis include the diurnal variation of symptoms, with prominent early morning stiffness, joint swelling due to synovitis in a symmetrical distribution in the small joints of the hand, and evidence of a systemic inflammatory response measured on blood tests including CRP and ESR.
In the early stages of disease, plain X-rays of the hands and feet are often performed to assess the presence of erosions or osteopenia, which can be monitored with treatment. In addition, ultrasound or MRI may be helpful in confirming the clinical findings of joint swelling, including synovitis or early erosions, which are indicators of joint damage that is likely to require early intervention.
RA is an autoimmune condition that is characterised by the presence of autoantibodies to rheumatoid factor (RhF) and anti-citrullinated (anti-CCP or ACPA) antibodies. The presence of these antibodies often predates the development of RA joint features by many years.
The development of RA is believed to be a multistep process (Figure 1.2):
•a genetic background such as the presence of susceptibility genes including alleles of the major histocompatibility complex (MHC) genes e.g. HLA-DR4, HLA-DR and PTPN22
•epigenetic factors such as the presence of autoantibodies
•associated environmental risks such as periodontal disease and smoking.
Figure 1.2. The development of rheumatoid arthritis
The factors described above all raise the likelihood of developing RA.
RA often develops as a systemic disease (meaning that it can affect the whole body) with the loss of immune tolerance, ongoing production of autoantibodies, proliferation of lymphoid tissue and activation of dendritic cells. Stimulation of the adaptive immune system leads to activation of several proinflammatory pathways, with initiation of cytokine cascades leading to changes focused around joints that include synovitis, bone erosions, inflammation and pain.
Because RA is a multisystem autoimmune condition, many changes occur including vascular inflammation, pain, inflammation, osteoporosis and metabolic changes, which can lead to extra-articular involvement.
Once the diagnosis has been established, care is based on rapid suppression of inflammation and pain based on the concept of ‘treat-to-target’.
1.4.1Non-pharmacological management
There is evidence supporting the role of early exercise therapy in RA, including for example hand therapy to strengthen and maintain muscles, tendons and ligaments, and physiotherapy. Exercise is recommended, including physiotherapy, hand therapy and occupational therapy (NICE guideline [NG100] Published date: July 2018).
1.4.2Pharmacological management
One of the early features of RA is pain and therefore pain management is a cornerstone of early treatment. Trial evidence shows that non-steroidal anti-inflammatory drugs (NSAIDs) are key to control early pain and inflammation. NICE guidance states that NSAIDs should be prescribed at the lowest dose possible for the shortest period of time in RA, ensuring that cardiovascular, renal and gastrointestinal risk factors are considered on a patient-by-patient basis (https://cks.nice.org.uk/nsaids-prescribing-issues#!scenario). NICE also recommends that gastroprotection in the form of a proton pump inhibitor (PPI) is cost-effective in people with conditions such as RA. In cases where several risk factors exist, e.g. cardiovascular, gastrointestinal in elderly patients, topical NSAIDs can be considered.
First-line therapy
First-li...