Although an abundance of research exists on working with students with autism, teachers need the practical strategies in Success Strategies for Teaching Kids With Autism to build successful programs and services for kids with autism.
The authors, seasoned classroom teachers and consultants for a large public school autism support program, look at ways teachers can apply best practices for teaching special needs students. They offer field-tested ideas for teachers to implement, covering topics such as managing difficult behaviors, teaching social skills, addressing communication difficulties, creating schedules, and organizing the classroom.
The book includes a detailed section on using applied behavior analysis, providing practical examples for teachers to employ in their own classrooms in order to modify student behaviors and increase learning. Including teacher-friendly overviews of the educational needs of students with autism and ideal teaching methods, the book also provides reproducible materials and photographs that show the strategies in action.
eBook - ePub
Success Strategies for Teaching Kids With Autism
- 254 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Success Strategies for Teaching Kids With Autism
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
EducationSubtopic
Behavioural ManagementCHAPTER 1
WHAT IS AUTISM?
DOI: 10.4324/9781003238294-1
A parent of a child with autism, in an anonymous posting on the Internet, describes autism as:
- Always
- Unique,
- Thoroughly
- Intriguing, and
- Sometimes
- Mysterious.
In the same passage, the author states that autism has brought Anger and rage, Unbelief and denial, Tears and sadness, Isolation and loneliness, and then Solace and peace. The author ends with thoughts of rejoicing in the child’s successes and delighting in the child’s Magic smile (Let’s Beat Autism Now, n.d.; see http://www.letsbeatautismnow.com/Poems.html for similar parent writings on this disorder).
In our experiences as teachers, we have found children with autism to be wonderful and fascinating. We have been privileged to participate in the many amazing achievements of our children and we have celebrated with their families. But, we also have shared in some of the pain, sorrow, and frustration experienced by the families and, perhaps most importantly, we have learned much from the challenges of helping children with this puzzling condition.
Autism is a complex spectrum disorder characterized by impairments in social interaction, communication, and behavior. The label autism spectrum disorder (ASD), an umbrella term, frequently is used to describe a continuum of features ranging from mild to severe. Each person with a diagnosis of ASD has a unique combination of characteristics related to verbal and nonverbal language (communication), interacting with others (social skills), and repetitive, narrow, and restricted interests (behavior). In individuals, these characteristics are presented in varying degrees of severity and result in different levels of functioning.
Autism spectrum disorders are considered to be neurobiological and generally are diagnosed by a team of professionals, including medical personnel. They also are described as developmental disabilities, meaning they usually are evident by 3 years of age. These neurobiological, developmental diagnoses of ASDs have lifelong influences on how individuals communicate their ideas and feelings, how they develop relationships with others, and how they participate in their environments.
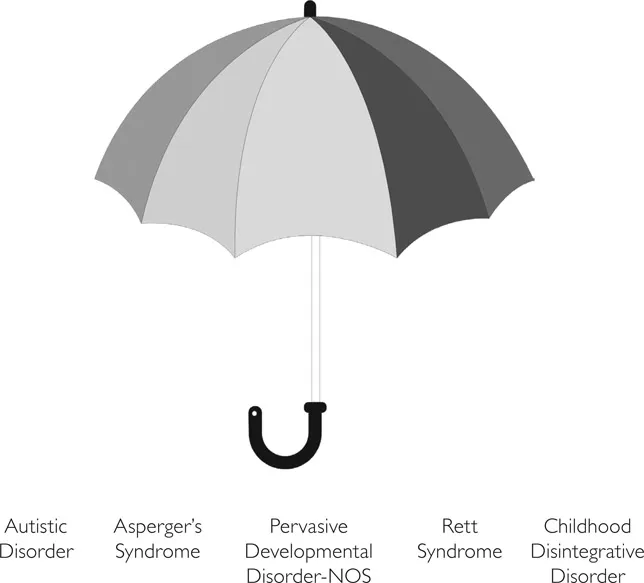
The term ASD often is used interchangeably with Pervasive Developmental Disorder (PDD). PDD also is an umbrella term (see Figure 2) encompassing the five disorders in the text revision of the fourth edition of the Diagnostic and Statistical Manual (DSM-IV-TR; American Psychiatric Association, 2000). Sometimes, ASD is used to refer only to three of the disorders: autism, Asperger’s syndrome, and Pervasive Development Disorder-Not Otherwise Specified (PDD-NOS). The prognosis for each of these three disorders is quite favorable in that, with effective treatment, individuals make significant progress. Other times, ASD also is considered to encompass two other disorders: Rett syndrome and childhood disintegrative disorder. Both of these are progressive disorders, describing individuals who start with a period of typical development and then enter a regressive phase. The prognosis for these two disorders is not as promising.
In the following pages, additional information is provided for each of the five disorders. Descriptions of children are presented to help explain how the disorder may affect individuals.
AUTISM
Autism (also called autistic disorder) is a complex condition diagnosed by observation and analysis of a person’s behavior patterns. It is a spectrum disorder, meaning it includes individuals with widely varying abilities and unique combinations of behavioral deficits and excesses. A complete evaluation of language, cognition, and behavior, as well as physical and neurological assessments, are necessary for a formal diagnosis. A good evaluation process involves consultations from a physician, psychologist, and speech-language pathologist, and parent information regarding developmental history and current functioning.
There is general agreement that autism is a neurological disorder affecting brain functioning and that it is a developmental disorder, usually diagnosed before the age of 3. People with autism often have difficulty with verbal and nonverbal communication and social interactions along with restricted interests, repetitive behaviors, and resistance to change.
Case Study of Autism: Mark
Mark was diagnosed with autism at age 2. From birth he had typical development, sitting at about age 6 months and walking at about a year. At 14 months he was consistently imitating sounds and actions, verbalizing while pointing to things he wanted and babbling. He clearly asked for mama, daddy, ball, and play, and occasionally put two words together like “Daddy go.” By 18 months he was walking on his tiptoes, wringing his hands, and crying instead of communicating. He no longer used understandable words and he stopped interacting with people.
When Mark was diagnosed, he had significant delays in social interaction such as avoiding eye contact and running away from people. Not only did he lose his ability to communicate with others, he showed no understanding of spoken language. He did not follow even simple directions. Between the ages of 2 and 3, Mark developed very frequent hand movements such as wringing his hands and twisting his fingers. His interest in toys was limited to waving them in front of his eyes.
At age 3, Mark began receiving intensive Discrete Trial Training (DTT) and quickly regained his ability to follow directions. He also learned to match and to name objects and pictures. In spite of intensive interactive instruction, Mark continued to show little interest in communicating with people. His restricted interests limited his opportunities to play with his brothers and yielded even fewer activities with neighbors and schoolmates. By age 6, Mark’s expressive vocabulary was more than 1,000 words; however, he still had little interest in interacting with others and often communicated with whining and crying rather than talking.
Today, Mark is improving in his abilities to listen to and communicate with others. His interests are widening as he has developed a passion for watching movies and playing video games. His ability to read words is providing his teachers an opportunity to use many of the strategies in this book to help him increase his interactions with others.
ASPERGER’S SYNDROME
The diagnosis of Asperger’s syndrome is made with a thorough analysis of the history of the person’s development of social and language skills and assessments and observation of an individual’s behaviors. A true diagnosis of Asperger’s syndrome (also called Asperger Disorder) is made when there is impairment in social interaction and unusual patterns of behavior along with no significant delay in language or cognitive development.
The impairment in social interaction is characterized by difficulties with tasks such as understanding nonverbal social cues, peculiarities in speech and language, recognizing and communicating emotions, making friends and maintaining peer relationships, and sharing enjoyment, interests, and achievements with others. The patterns of behavior can include restricted interests and activities; preoccupation or obsession with a particular subject; strong dislike for change and inflexible adherence to routines or rituals; unusual sensitivity to sound, light, or touch; or awkward, repetitive mannerisms.
People with Asperger’s syndrome may demonstrate clumsy and uncoordinated motor movements and repetitive behaviors or rituals. Sometimes, people with Asperger’s syndrome have an impaired ability to be empathetic with other people and can be thought of as egotistical, selfish, or uncaring.
Case Study of Asperger’s Syndrome: Michael
Michael’s language developed early and quickly, but his motor milestones were slightly delayed. At age 2, he was speaking in complete sentences with a remarkably advanced vocabulary. By age 3, he was reading first-grade-level books and adding and subtracting double-digit math problems. These academic tasks became his favorite activities, and he often would whine or scream when he was interrupted from them. He would spend some time interacting with others while playing with his extensive collection of trains; however, whenever free to choose, he spent both his academic and play time alone.
Michael was very anxious in unstructured situations and quite uncooperative during group play times in his daycare program. Rather than interact with others, he played by himself and shouted at children who attempted to play with him.
Michael did not respond appropriately to social cues. For example, he talked when it was quiet time and often stayed silent when asked a question. In addition, his tone of voice frequently did not match the situation. When he was 5 years old, he spoke like an adult and his vocabulary and intonation indicated to others that he was much older, almost adult-like.
Michael was very sensitive to smells and it was difficult for him to eat in the cafeteria. He was very anxious, even fearful, of situations like elevators or escalators and hated most art projects. Michael seemed uncomfortable conversing with classmates and happiest when working on the computer. He did not seem to know how to approach small groups of children to join an activity and although he had plenty of language skills, he often was unsuccessful in beginning and ending conversations. He seemed most comfortable talking about trains and would talk about trains as long as anyone would listen.
Today, Michael is achieving well in school. His teachers and parents have used the strategies in this book, and Michael is becoming more comfortable interacting with others.
PERVASIVE DEVELOPMENTAL DISORDER-NOT OTHERWISE SPECIFIED
The third disorder under the PDD umbrella is Pervasive Developmental Disorder-Not Otherwise Specified (PDD-NOS). PDD-NOS is a diagnosis that sometimes is referred to as atypical autism or atypical personality development.
The diagnosis of PDD-NOS is used when a child does not have the complete features of autism or a more clearly defined pervasive developmental disorder. The relatively broad definition for this mixed group of children presents problems for diagnosing this condition and results in a very heterogeneous population. In PDD-NOS, there is noticeable impairment of social interaction, communication, and/or stereotyped behavior patterns, usually recognizable before a child is 3 years old. However, in children with PDD-NOS, the deficits may not be as severe or the impairments may not occur in configurations that would meet the criteria for an autism diagnosis. For example, one child may receive a diagnosis of PDD-NOS due to having only a few mild symptoms. Another child might have very significant language or social impairments, but not have the unusual behavior patterns necessary for a diagnosis of autism. In addition, while a child’s profile might seem to fit the criteria, many of these behaviors are developmental and, for some children, the symptoms might just be part of a slightly unusual growth pattern, rather than PDD-NOS.
Case Study of PDD-NOS: Mindy
Mindy was the oldest of two children. She was a difficult baby who was not easy to console, but her developmental milestones for both communication and motor skills seemed appropriate. She enjoyed social interaction but was easily overstimulated. As a toddler, Mindy exhibited high sensitivity to sounds, smells, and touch and at times of excitement engaged in hand flapping.
Her parents sought evaluation when she was 4 years of age because of difficulties in preschool. Her communicative and cognitive functions were within the normal range and she did not have the full features of autism. Mindy received a diagnosis of PDD-NOS due to her social problems with peers and her insistence on routines. When upset by changes in her environment, Mindy was slow to respond to her parents’ reassurances and often would stay agitated for hours at a time. Mindy was enrolled in preschool where she made significant gains in social skills and continued her academic success. Throughout elementary school, problems with peer interactions persisted and her academic progress slowed. Mindy resisted changes to her routine by continuing to follow the previous pattern of activity. When asked to change or to do something new, Mindy would hum, rock, and spin while refusing to comply with instructions. In elementary school, Mindy continued to have difficulties with social interaction, tended to enjoy solitary activities, and described herself as a loner.
Today, Mindy is using many of the strategies in this book to communicate and interact with others. She seems happier and more comfortable in school and plays with friends in structured play groups at home.
CHILDHOOD DISINTEGRATIVE DISORDER
Children with childhood disintegrative disorder typically show normal development for at least the first 2 years of life. This includes typical development of motor skills, verbal and nonverbal communication, social interaction and play skills, and self-care skills. Before the age of 10, there is regression in the ability to say words or sentences (expressive language), the ability to understand verbal and nonverbal communication (receptive language), and the ability to interact with others (social skills). There also may be loss of motor skills, bowel and bladder control, and self-care skills (adaptive behavior). These changes may occur suddenly and quickly, possibly in a few days or weeks, or they may occur gradually over a period of several months.
The loss of communication skills may include a reduction in spoken language, a decrease in the ability to initiate or sustain a conversation, an increase in repetitive use of language, and a decline in imaginative or make-believe play. The loss of abilities in social interaction skills may include impairment in the ability to respond appropriately to the nonverbal behaviors of others, failure to develop peer relationships, and a lack of social or emotional reciprocity. In this stage, children often have an inability to recognize, understand, and respond to social cues and feelings of others. The loss of motor skills involves a declining ability to move the body in a purposeful way. This may be accompanied by the development of repetitive and stereotyped patterns such as hand flapping, rocking, and spinning; the development of specific routines and rituals; difficulty with transitions or changes in routine; maintaining a fixed posture or body position; and preoccupation with certain objects or activities.
Case Study of Childhood Disintegrative Disorder: John
John’s early history was within normal limits. By age 2 he was speaking in sentences and his development appeared to be proceeding appropriately. He was a cheerful toddler—smiling, developing language, and using the toilet. Then, gradually, he began losing interest in other people and his use of language seemed to decrease. He developed self-stimulating behavior such as flapping his hands and rocking and stopped using the bathroom.
Previously, John accepted hugs as reassurance from his parents, but eventually lost the ability to be consoled and tensed his muscles every time he was touched. At age 30 months John stopped all attempts at communication and was no longer toilet trained. He no longer showed interest in social interaction and his self-stimulatory actions became almost constant. A comprehensive medical examination failed to reveal any physical conditions to explain his regression and all medical notes described features of autism. At age 9 he occasionally spoke single words, pulled away from hugs and touch, and spent all unengaged time in self-stimulating behaviors.
Today, John is responding to visual supports recommended in this book. Although he is still uncomfortable with too much touch, he allows and tolerates interactions that are predictable to him. He responds well to routines and is particularly responsive to high-five gestures from others.
RETT SYNDROME
Rett syndrome (also known as Rett’s disorder) is characterized by an initial period of normal development followed by a loss of communication skills and deliberate hand movements. It is the only one of the PDD conditions that has a period of rapid deterioration followed by stabilization and sometimes includes periods of increases in eye contact and reductions of stereotypical hand movements. Because of these periods of stabilization, most experts now agree that it is a developmental disorder, rather than a degenerative disorder. Rett syndrome often is mistaken for autism, cerebral palsy, or mental retardation, so a precise developmental history is critical to an accurate diagnosis.
Rett syndrome occurs almost exclusively in females and occurs in a variety of racial and ethnic groups worldwide. In earlier times it was thought that males with Rett syndrome did not survive long enough to be born. Researchers have now identified a genetic flaw in some children with Rett syndrome. Although the great...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Contents
- Acknowledgments
- Introduction
- Chapter 1 What Is Autism?
- Chapter 2 What Makes a Successful Education Program for Children With a Diagnosis of ASD?
- Chapter 3 What Is ABA?
- Chapter 4 How Can ABA Principles Be Implemented in Education Programs?
- Chapter 5 Creating an Evidence-Based Classroom
- Chapter 6 Strategies for Addressing the Major Characteristics of ASD in the Classroom
- Chapter 7 Putting It All Together
- Conclusion
- References
- About the Authors
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Success Strategies for Teaching Kids With Autism by Wendy Ashcroft,Sue Argiro,Joyce Keohane in PDF and/or ePUB format, as well as other popular books in Education & Behavioural Management. We have over 1.5 million books available in our catalogue for you to explore.