The eBook version of this title gives you access to the complete book content electronically*. Evolve eBooks allows you to quickly search the entire book, make notes, add highlights, and study more efficiently. Buying other Evolve eBooks titles makes your learning experience even better: all of the eBooks will work together on your electronic "bookshelf", so that you can search across your entire library of Dentistry eBooks.*Please note that this version is the eBook only and does not include the printed textbook. Alternatively, you can buy the Text and Evolve eBooks Package (which gives you the printed book plus the eBook). Please scroll down to our Related Titles section to find this title.A popular and concise textbook of restorative dentistry for the dental student, illustrated in colour throughout. The book covers the specialties of restorative dentistry - operative dentistry, endodontics, periodontics and prosthetic dentistry - in a single volume.- Treatment planning section demonstrates the integration of the main constituent specialties in the treatment of patients with multiple problems.- Realistic case studies illustrate useful day-to-day practice.- High quality colour illustration throughout with free use of key point boxes and tables.- Increased length allows greater coverage of new and important topics- New chapters on cariology and on immediate and complete dentures- Occlusion chapter completely rewritten and simplified- Expanded and more detailed chapter on examination of the patient- New sections at the end of each chapter covering more advanced techniques
eBook - ePub
Restorative Dentistry
- 244 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Restorative Dentistry
About this book
Information
Chapter 1
Introduction to restorative dentistry
Keeping teeth is important for many functions, such as eating and speech, whilst in our present society good aesthetics are a high priority for the majority of people. A realistic outcome of dentistry must be a healthy comfortable mouth with sound intact teeth. Dental care must also be designed to prevent any future problems and to help to maintain this healthy environment. Restorative dentistry involves the care of patients who require restoration of the oral and dental tissues. This area of dentistry crosses many of the traditional departments that exist in teaching hospitals throughout the world and includes the disciplines of periodontology, operative dentistry, endodontics, and fixed and removable prosthodontics. Other specialities, such as oral surgery and orthodontics, are often involved in the planning of restorative care.
Although the restoration of the oral tissues requires technical skills, the clinician is intimately involved in the decision-making process. A patient should receive investigations that lead to a correct diagnosis. The clinician reaches the diagnosis after careful history-taking and examination of the patient. Only then can a treatment plan be drawn up which helps to achieve oral stability. The clinician should be an expert in all the disciplines that make up restorative dentistry, but should also be able to integrate them in a sensible order and not as compartmentalised procedures.
The subject areas in the book are arranged in a traditional order with periodontology at the start, and fixed and removable prosthodontics towards the end. The last chapter hopes to show, with the use of case studies, that the progress of patient care often does not follow such steps. Patients often require intervention with an immediate partial denture towards the beginning of treatment prior to the instigation of periodontal care. A patient with irreversible pulpitis requires pain relief, which involves the use of endodontic care. The fracture of a tooth needs temporising or, when occurring to the anterior teeth, a temporary crown or other restoration is required. The list of interactivity between the traditional disciplines is long and shows the diverse nature of treatment planning that will take place.
Prevention of damage to the tooth is a fundamental part of restorative care. This will range from motivating patients to clean their teeth effectively, to monitoring their diet and giving appropriate advice. An increase in the demand for more advanced treatment reflects changes in patient expectation, with a reluctance to accept tooth loss and an increasing demand for advanced restorative treatment. There is often a need for comprehensive periodontal assessment and for advice and treatment of periodontal problems, which in the past have received insufficient attention. Tooth wear is an increasing problem that causes sufferers concern, requiring careful assessment and sometimes complex reconstructive techniques to avoid future treatment and failure.
The restorative dentist is the leader of the dental team and is responsible for the management of nursing and hygiene care and laboratory support. Such a dentist must be active in the field of clinical audit, establishing indices of treatment need and measures to assess the outcome of treatment procedures. Clinical governance is defined as corporate accountability for clinical performance and is about standards of quality. The restorative dentist should take part in continuing professional development programmes and offer leadership to develop and improve the quality of restorative dentistry care.
Chapter 2
The healthy mouth
The mouth is a highly specialised organ whose complex topographical anatomy reflects the diverse activities that it must perform.
LIPS AND CHEEKS
The lips are muscular structures surrounding the opening of the mouth. Externally they are covered with skin which is tightly bound down to the underlying connective tissue and muscle, and which contains sweat glands, hair follicles and sebaceous glands.
The inner surface of the lips is covered with stratified squamous epithelium, tightly attached to the underlying connective tissue and muscle. The epithelium is thin, and through it the underlying blood vessels are visible. The surface is irregular with slight prominences caused by the presence of large numbers of small mixed salivary glands.
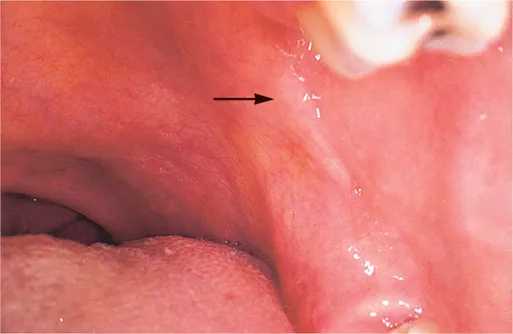
The mucous membrane of the cheeks is also tightly bound down to the underlying connective tissue and muscle. To allow for stretching, and accommodation to the movements of the mouth and cheeks, the mucous membrane has a finely wrinkled form in the resting state. Superiorly and inferiorly, the boundaries of the inner surface of the cheek are the buccal sulci of the maxillary and mandibular alveolar processes. Posteriorly, the pterygomandibular raphe — a fibrous tissue band — stretches from the pterygoid process to the retromolar pad of the mandible (Fig. 2.1). Anteriorly the mucous membrane is continuous with that of the lips.
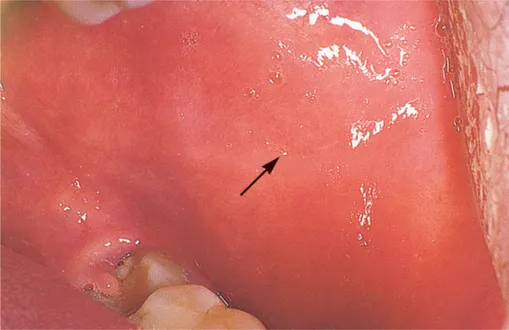
In the maxillary second molar region, the mucous membrane of the cheeks is pierced by a duct — the parotid duct — which ends as a papilla of variable size. Further down in the cheek, level with the occlusal surfaces of the teeth, there is often a slightly raised, horizontal whitish band (Fig. 2.2). This is a band of keratinisation produced by chronic trauma from the teeth. While often barely noticeable, it can be pronounced and lead to confusion with other, pathological, types of white lesion.
Posteriorly and in line with the corners of the mouth there are often a small number of ectopic sebaceous glands. These are of no significance but can be alarming when present in large numbers. At times a large area may be covered by such sebaceous glands which appear as yellowish spots — Fordyce’s spots — and these can cause anxiety when noticed for the first time.
Superiorly and inferiorly, the mucous membrane which is bound down to the underlying muscle loses its attachment and is reflected onto the bone of the alveolar processes. The zone of reflection — the sulcus — must allow for the mobility of the cheeks and the mucous membrane is attached to the underlying structures only by loose connective tissue. The sulci are horseshoe-shaped and are divided into buccal and labial sections related to the cheeks and lips, respectively. Where the sections join, their continuity is interrupted by a variable number of sickle-shaped fraenal attachments. The most consistently present of these are in the upper midline (Fig. 2.3), which is usually well developed, and the lower midline, which is less so. Smaller fraenal attachments are usually found in the upper and lower sulci in the canine/premolar region. Fraenal attachments do not contain muscle and consist only of mucous membrane separated by a little thin fibrous tissue.

The upper midline fraenal attachment may be enlarged and have a fibrous insertion into the maxilla which, if it is associated with lack of bony fusion, may be an orthodontic problem. Fraena may also be a contributory factor in periodontal disease by interfering with plaque removal, and in the edentulous patient where the denture base may need to be deeply notched to provide relief over the fraenum. The fraenal attachment may then require surgical removal.
ALVEOLAR PROCESSES
The mucous membrane covering the alveolar processes is of two types. That part which is continuous with the sulcus, the alveolar mucosa, is thin and loosely attached to the underlying bone by thin connective tissue. This allows it to accommodate to the free movement of the lips and cheeks and permits the painless deposition of local anaesthetic into the underlying connective tissue. The thinness and the plentiful blood supply give it a ...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- Contributors
- Preface
- Acknowledgements
- Chapter 1: Introduction to restorative dentistry
- Chapter 2: The healthy mouth
- Chapter 3: Examination of the patient and treatment planning
- Chapter 4: Inflammatory periodontal diseases
- Chapter 5: Management of inflammatory periodontal diseases
- Chapter 6: Occlusion
- Chapter 7: Caries and other reasons for restoring teeth
- Chapter 8: Restoration of teeth (simple restorations) and preventative dentistry
- Chapter 9: Management of pulpal and periradicular disease
- Chapter 10: Restoration of teeth (complex restorations)
- Chapter 11: Treatment of tooth substance loss
- Chapter 12: The principles of tooth replacement
- Chapter 13: Integrated treatment planning
- References and suggested further reading
- Index
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Restorative Dentistry by A. Damien Walmsley,Trevor F. Walsh,Philip Lumley,F. J. Trevor Burke,A. C. Shortall,Richard Hayes-Hall,Iain Pretty in PDF and/or ePUB format, as well as other popular books in Medicine & Dentistry. We have over 1.5 million books available in our catalogue for you to explore.