Offering authoritative guidance and a multitude of high-quality images, Facial Trauma Surgery: From Primary Repair to Reconstruction is the first comprehensive textbook of its kind on treating primary facial trauma and delayed reconstruction of both the soft tissues and craniofacial bony skeleton. This unique volume is a practical, complete reference for clinical presentation, fracture pattern, classification, and management of patients with traumatic facial injury, helping you provide the best possible outcomes for patients' successful reintegration into work and society.- Explains the basic principles and concepts of primary traumatic facial injury repair and secondary facial reconstruction.- Offers expert, up-to-date guidance from global leaders in plastic and reconstructive surgery, otolaryngology and facial plastic surgery, oral maxillofacial surgery, neurosurgery, and oculoplastic surgery.- Covers innovative topics such as virtual surgical planning, 3D printing, intraoperative surgical navigation, post-traumatic injury, treatment of facial pain, and the roles of microsurgery and facial transplantation in the treatment facial traumatic injuries.- Includes an end commentary in every chapter provided by Dr. Paul Manson, former Chief of Plastic Surgery at Johns Hopkins Hospital and a pioneer in the field of acute treatment of traumatic facial injuries.- Offers videos that clarify surgical technique, including intraoperative guidance and imaging; transconjunctival approach to the orbit and reconstruction of a zygomaticomaxillary complex fracture; calvarial bone autograft splitting; dental splinting; a systematic method for reading a craniofacial CT scan; and more.- Features superb photographs and illustrations throughout, as well as evidence-based summaries in current areas of controversy.- Enhanced eBook version included with purchase. Your enhanced eBook allows you to access all of the text, figures, and references from the book on a variety of devices.
eBook - ePub
Facial Trauma Surgery E-Book
From Primary Repair to Reconstruction
- 512 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Facial Trauma Surgery E-Book
From Primary Repair to Reconstruction
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
Plastic & Cosmetic MedicineSection 1
Primary Injury
1.1
Assessment of the Patient With Traumatic Facial Injury
Arthur J. Nam, Edward H. Davidson, Paul N. Manson
Background
Incidence of Facial Trauma in the United States and Worldwide
The spectrum of facial trauma includes soft tissue and bone, and ranges from the simple to the complex. Epidemiology varies with local and global demographic factors and reflects a complex interplay of influences, including those related to the environment, economics, age, gender, and mechanism of injury. Any understanding of the incidence of facial trauma is further confounded by the presumptive underreporting and treatment of minor injuries. As a result, the plethora of data is often conflicting. Nonetheless, the incidence of facial fractures presenting to the emergency room is approximately 500,000 per year in the United States, with nasal fractures likely the most common, followed by mandible fractures.1 These commonly occur in males more than females, are most frequent in the second and third decades of life, and are most frequently the result of altercations, assaults, falls, work or home accidents, and motor vehicle or motorcycle collisions (MVCs). While many studies cite mandible fractures as being more common than nasal fractures, this has been attributed to a sampling bias favoring inpatient admissions or requirement for in-hospital treatment rather than capturing all emergency room presentations. Several older studies show higher rates of injury from MVCs, prior to the mandatory implementation of airbags and restraining devices.2 Despite this, MVCs remain the most important cause of facial trauma all over the world. Global trends also reflect an increase in the male/female injury ratio in countries where the social custom is for women to be more confined to the home.3 Associated soft tissue trauma is the most common concomitant injury, occurring in approximately 30% of facial fractures. Concomitant fractures of the skull, upper limbs, and associated areas are estimated to occur in around 25% of facial fractures; these include intracranial injuries in 12%–45.5%, and associated cervical spine injury with facial injury in up to 9.7%.1,4 One must therefore always exclude brain and cervical spine injuries in the patient with facial injuries as trauma is often a geographic injury to the head and neck. Missed injuries of the spine, extremities, and pelvis are also frequent (10%) and are easily missed.
Patterns of Facial Trauma and Causes
Patterns of facial injuries may be subdivided into soft tissue, bony skeleton, and/or dentoalveolar trauma. Descriptions can also be made based on location in facial thirds: the upper third (including the frontal bone, frontal sinuses, and orbital roofs), middle third (including the orbit, nose, malar region, and maxilla), and lower third (including the mandible and its dentition) (Fig. 1.1.1). Blunt trauma can result in relatively predictable fracture patterns due to the presence of facial buttresses and resultant functional skeletal units (Fig. 1.1.2).5 Injury to the upper third may reveal frontal sinus fractures, which require the determination of whether injury affects the inner table, outer table, or both, degree of displacement, and the presence of nasofrontal outflow tract obstruction.6 Midface fracture patterns may include the characteristic Le Fort fracture patterns, but are more frequently asymmetric and more extensive on the side of the force application, or orbitozygomaticomaxillary complex (OZMC), orbital, nasal and naso-orbito-ethmoid (NOE) fractures in isolation or in combination. Lower third facial fractures, i.e., those of the mandible, also demonstrate reproducible patterns. The most prevalent site of mandibular fracture reported in the literature is variable, though mandibular angle and condyle are the most frequently cited.7 Based on the mandibular “ring” concept, mandibular fractures have conventionally been thought to involve at least two sites, however, unifocal mandibular fractures commonly occur. Common multifocal patterns include mandibular body and contralateral angle/ramus/condyle, angle and contralateral parasymphysis, symphysis/parasymphysis, and bilateral condyle. True panfacial fractures involve all thirds of the face simultaneously and are less involved on the contralateral side, both in terms of fracture extent and comminution.8 These fracture patterns differ depending on mechanism, with most panfacial fractures usually resulting from MVCs and, less commonly, from gunshot wounds (GSWs). Sports injuries typically are isolated to the mandible or upper midface, and assaults are predictive of isolated mandible, midface or zygoma fractures. MVCs and GSWs each predict a higher severity of injury than assaults, falls, or sports injuries.9,10
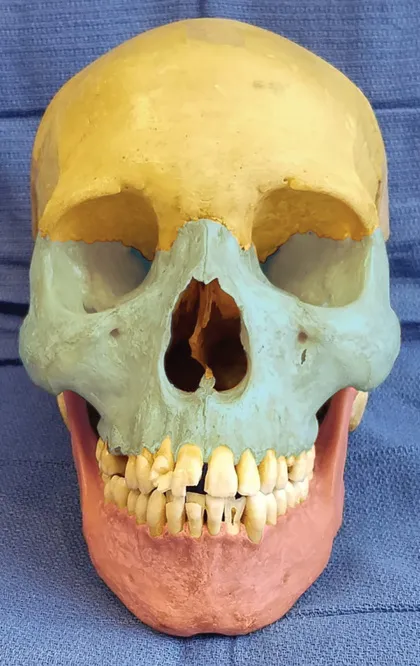
Fig. 1.1.1 Facial skeleton in thirds: upper (yellow), middle (blue), lower (pink).

Fig. 1.1.2 Transverse (blue), vertical (red), and sagittal (green) buttresses of the facial skeleton. (From Prein J, Ehrenfeld M, Manson PN, editors. Principles of internal fixation of the craniomaxillofacial skeleton: trauma and orthognathic surgery. AO Foundation, Thieme; 2012, Fig. 1.3.1-5, p.24.)
Patterns of facial trauma in the pediatric population differ from those in adults. Facial fractures are relatively less common in children due to parental supervision as well as intrinsic anatomical factors such as larger fat pads, decreased pneumatization of sinuses, increased skeletal flexibility secondary to more malleable bone stock, and compliant sutures. The large cranium partially shields the rest of the face from injury. Atypical craniofacial fracture patterns precede the Le Fort patterns seen in adulthood and as an incompletely pneumatized frontal sinus transmits energy directly from the site of impact to the supraorbital foramen and then to the orbit, superior NOE and anterior maxillary wall or zygoma.11,12 Younger patients are at higher risk of dentoalveolar trauma, including crown fractures (the most common injury), luxations, avulsions, subluxations, root fractures, and intrusions, with approximately one-third occurring in those younger than 10 years of age. These most often result from activities of daily living, play, MVCs, and sports.13
The relative incidence of fracture patterns is debated; mandible fractures are often cited as the most common pediatric facial fracture, accounting for 20%–50% of all pediatric facial fractures.14–17 Anatomical distribution varies with age; isolated condylar fracture incidence decreases, while body and angle fractures increase.18 Others have reported ...
Table of contents
- Cover image
- Title Page
- Table of Contents
- Copyright
- Video Contents
- Foreword
- Preface
- List of Contributors
- Acknowledgments
- Dedication
- Section 1 Primary Injury
- Section 2 Pediatric Facial Injury
- Section 3 Secondary Reconstruction and Restoration
- Appendix 1 Evidence-Based Medicine
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Facial Trauma Surgery E-Book by Amir H Dorafshar,Eduardo D Rodriguez,Paul N Manson, Amir H Dorafshar, Eduardo D Rodriguez, Paul N Manson in PDF and/or ePUB format, as well as other popular books in Medicine & Plastic & Cosmetic Medicine. We have over 1.5 million books available in our catalogue for you to explore.