Practical, user-friendly, and to the point, the newly updated Kaplan's Essentials of Cardiac Anesthesia, 2nd edition focuses on the most common topics and clinically applicable information in cardiac anesthesia today. Designed for residents, nurses, and clinicians seeking quick, high-yield answers rather than the encyclopedic information commonly found in larger references—in fact, its concise format makes it easy to complete a section in a single sitting. For an initial introduction to cardiac anesthesia, nothing compares to Kaplan's Essentials!- Trusted authorities deliver the key cardiac anesthesia knowledge you need to know.- A concise, user-friendly format and key points boxes in each chapter help you quickly locate crucial information.- Annotated references guide you to the most practical additional resources.- A portable size and clinical emphasis facilitates and enhances bedside patient care.- Designed as a companion to Kaplan's Cardiac Anesthesia.- Includes new topics vital to the current practice of cardiac anesthesiologists, such as transesophageal echocardiography; percutaneous valve procedures; new pacemakers and automatic internal defibrillators used for cardiac resynchronization therapy; left ventricular assist devices and extracorporeal membrane oxygenation therapy of heart failure; and patient safety issues.- Focuses on today's most current and relevant therapies, including New Cardiac Drugs, and Heart Mate, Heart Ware, and Impella LVADs.- Describes care of the cardiac patient in Hybrid Operating Rooms, Catheterization Laboratories, and Electrophysiology Laboratories, as well as the Cardiac Operating Rooms.- Perfectly suited for residents, fellows, nurse anesthetists and anesthesiologists in practice.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Alexander J.C. Mittnacht MD, Martin J. London MD, John D. Puskas MD, Joel A. Kaplan MD, CPE, FACC
Key Points
1. Guideline updates emphasize the efficacy of surgical approaches to myocardial revascularization in patients with multivessel coronary artery disease.
2. Perioperative risk reduction includes careful consideration of all of the patient's relevant antihypertensive, antiplatelet, and antianginal medications.
3. Significant valvular abnormalities in patients scheduled for coronary revascularization should be evaluated and considered in surgical planning.
4. Off-pump coronary artery bypass surgery is an established alternative to on-pump myocardial revascularization (ie, coronary artery bypass grafting [CABG]). The choice and outcomes of either approach are highly surgeon dependent. Despite apparent advantages of avoiding cardiopulmonary bypass (CPB), evidence from large prospective trials enrolling mostly low-risk patients has not shown clear reductions in mortality with an off-pump approach.
5. Possible indications for pulmonary artery catheter use in CABG surgery include patients with pulmonary hypertension, right-sided heart failure, or severely impaired ventricular function, particularly those who require postoperative cardiac output monitoring.
6. Fast-tracking, including early extubation and mobilization, has been almost universally adopted for patients undergoing myocardial revascularization.
7. Anesthetic drugs, especially inhaled anesthetic agents, may help to ameliorate myocardial injury associated with CPB and aortic cross-clamping by their preconditioning and postconditioning effects. However, the magnitude of these effects on outcome remains controversial.
The role of the cardiac anesthesiologist in the perioperative care of patients undergoing myocardial revascularization continues to evolve. Achievements of the past two decades include providing safe anesthesia that allows rapid recovery and optimizing monitoring that includes the establishment of transesophageal echocardiography (TEE) as a standard of care in the cardiac operating room. More recent developments in patient care include the introduction of a perioperative surgical home, which affects the management of patients undergoing myocardial revascularization. The anesthesiologist is vitally important in the multidisciplinary approach to patient care. Optimal perioperative care requires close collaboration and coordination between the various specialties involved on the heart team. The process begins with the decision to proceed to surgery and continues with preoperative optimization, state-of-the-art perioperative and postoperative care, and rehabilitation after hospital discharge. Beyond safe anesthesia technique, the anesthesiologist must be well versed in all areas of perioperative management for patients with coronary artery disease (CAD). This includes advances in pharmacologic risk reduction, new surgical techniques, and anesthetic management and monitoring techniques to improve patient outcomes.
Epidemiology
According to the American Heart Association Heart Disease and Stroke Statistics, most recently updated in 2014, epidemiologic data relevant to cardiovascular disease can be summarized as follows. Overall rates of death attributable to cardiovascular disease have declined 31%; for CAD, there was a 39.2% decrease from 2000 to 2010. This was partially attributed to improvements in acute treatment of patients with acute coronary syndromes (ACSs), secondary preventive therapies after myocardial infarction (MI), treatment of acute heart failure (HF), revascularization of chronic CAD, and other preventive therapies. However, the prevalence remains high, with cardiovascular disease accounting for 31.9% of all deaths in the United States. Based on current estimates, by 2030 43.9% of the US population will have some form of cardiovascular disease. Similarly, 15.4 million individuals had CAD in 2010; and ischemic heart disease causes approximately one of every six deaths in the United States. In 2010, 379,559 Americans died of CAD, and statistically, every 34 seconds one person in the United States has a coronary event.
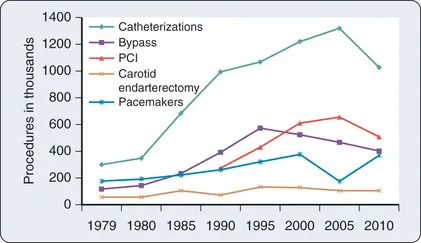
Between 2000 and 2010 the total number of inpatient cardiovascular procedures in the United States increased by 28%, with a total of 7,588,000 cardiovascular procedures performed in 2010. In 2010 an estimated 219,000 patients underwent 397,000 coronary artery bypass graft (CABG) procedures (Fig. 14.1). The in-hospital mortality rate for CABG declined by 50% despite an increase in the comorbidity index. CAD alone resulted in more than $44 billion in expenses, making it the most expensive condition treated. The total direct and indirect cost of cardiovascular disease and stroke was estimated to be $315.4 billion in 2010, more than for any other diagnostic group.
Fig. 14.1Trends in cardiovascular operations and procedures from 1979 to 2010 for inpatient procedures only. PCI, Percutaneous coronary intervention.(From Mozaffarian D, Benjamin EJ, Go AS, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics: 2015 update. A report from the American Heart Association. Circulation. 2015;131:e29.)
Pathophysiology of Coronary Artery Disease
Anatomy
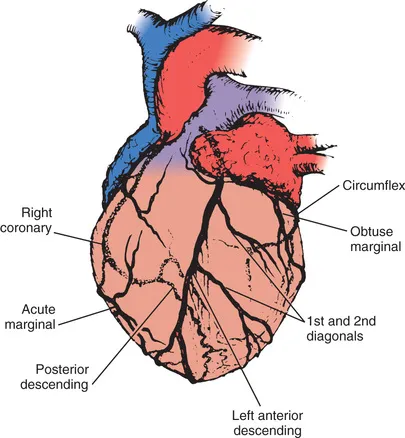
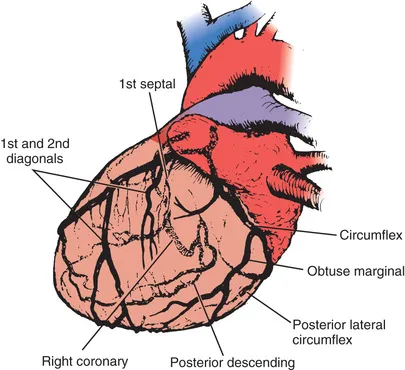
The anesthesiologist should be familiar with coronary anatomy if only to interpret the significance of angiographic findings. The coronary circulation and common sites for placement of distal anastomoses during CABG are shown in Figs. 14.2 through 14.4.
Fig. 14.2Thirty-degree left anterior oblique angiographic view of the heart, which best shows the right coronary artery. Lines indicate common sites of distal vein graft anastomoses.(From Stiles QR, Tucker BL, Lindesmith GG, et al. Myocardial Revascularization: A Surgical Atlas. Boston, Little, Brown; 1976.)
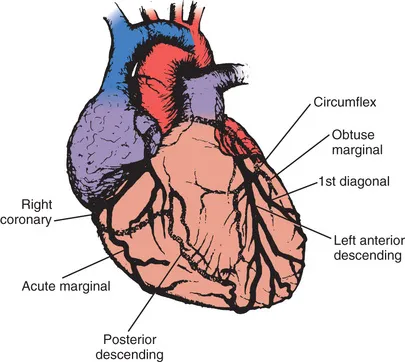
Fig. 14.3Ten-degree right anterior oblique angiographic view of the heart, which best shows the left main coronary artery dividing into the circumflex and left anterior descending arteries. Lines indicate common sites of distal vein graft anastomoses.(Modified from Stiles QR, Tucker BL, Lindesmith GG, et al. Myocardial Revascularization: A Surgical Atlas. Boston: Little, Brown; 1976.)
Fig. 14.4Seventy-five–degree left anterior oblique angiographic view of the heart, which best shows branches of the left anterior descending and circumflex coronary arteries. Lines indicate common sites of distal vein graft anastomoses.(Modified from Stiles QR, Tucker BL, Lindesmith GG, et al. Myocardial Revascularization: A Surgical Atlas. Boston: Little, Brown; 1976.)
The right coronary artery (RCA) arises from the right sinus of Valsalva and is best seen in the left anterior oblique view on coronary cine angiography. It passes anteriorly for the first few millimeters and then follows the right atrioventricular (AV) groove and curves posteriorly within the groove to reach the crux of the heart, the area where the interventricular septum (IVS) meets the AV groove. In 84% of cases, it terminates as the posterior descending artery (PDA), which is its most important branch because it is the sole supply to the posterosuperior IVS. Other important branches are those to the sinus node in 60% of patients and the AV node in approximately 85% of patients. Anatomists consider the RCA to be dominant when it crosses the crux of the heart and continues in the AV groove regardless of the origin of the PDA. Angiographers, however, ascribe dominance to the artery—right coronary or left coronary (ie, circumflex)—that gives rise to the PDA.
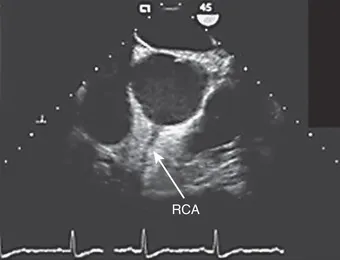
The vertical and superior orientation of the RCA ostium allows easy passage of air bubbles during aortic cannulation, cardiopulmonary bypass (CPB), or open valve surgery. In sufficient volume, myocardial ischemia involving the inferior left ventricular (LV) wall segments and the right ventricle may occur (Fig. 14.5). In contrast, the near-perpendicular orientation of the left main coronary ostium makes air embolization much less common.
Fig. 14.5The vertical and superior orientation of the right coronary artery (RCA) arising from the aortic root is identified by transesophageal echocardiography (TEE). The TEE transducer in the esophagus is at the top of the screen, and the patient's chest wall is at the bottom. Retained air preferentially enters the RCA, which may cause inferior ischemia, depending on the amount of air and the coronary perfusion pressure. Elevation of perfusion pressure using phenylephrine is often used to treat coronary air embolus. The left main coronary artery (not visible) arises at approximately 3 o'clock on this image.(Courtesy Martin J. London, MD, University of California, San Francisco, CA [www.ucsf.edu/teeecho].)
The left coronary artery arises from the left sinus of Valsalva as the left main coronary artery. It is best seen in a shallow right anterior oblique projection (see Fig. 14.3). The left main coronary artery courses anteriorly and to the left, where it divides in a space between the aorta and pulmonary artery. Its branches are the left anterior descending (LAD) artery and circumflex artery. The LAD passes along the anterior interventricular groove. It may reach only two-thirds of the distance to the apex or extend around the apex to the diaphragmatic portion of the left ventricle. Major branches of the LAD are the diagonal branches, which sup...
Table of contents
Cover image
Title Page
Table of Contents
Copyright
Dedication
Contributors
Preface
Section I Preoperative Assessment and Management
Section II Cardiovascular Physiology, Pharmacology, Molecular Biology, and Genetics
Section III Monitoring
Section IV Anesthesia for Cardiac Surgical Procedures
Section V Extracorporeal Circulation
Section VI Postoperative Care
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Kaplan's Essentials of Cardiac Anesthesia E-Book by Joel A. Kaplan in PDF and/or ePUB format, as well as other popular books in Medicine & Anesthesiology & Pain Management. We have over 1.5 million books available in our catalogue for you to explore.