Edited and authored by leading international experts, Distal Radius Fractures: Evidence-Based Management provides a state-of-the-art overview of diagnosis and management based on today's best practices. Each chapter focuses on one key issue, offering a challenging case and then questioning the reader in an engaging fashion to provide the best available evidence on each topic. Practical and easy to read, this innovative text is a useful resource for all residents, physicians and surgeons who manage fractures.- Combines current best practices with the knowledge and experience of a global team of expert contributing authors, with a focus on practical use in applying the evidence.- Covers need-to-know topics such as anatomy and biomechanics, diagnostic management, acute fracture management, management of pediatric and elderly fractures, and more.- Includes valuable case scenarios, technical tips and tricks, and pearls and pitfalls.- Features high-quality illustrations including CT scans, x-rays, and clinical photographs.- Consolidates the latest evidence on distal radius fractures into one convenient resource.
eBook - ePub
Distal Radius Fractures
Evidence-Based Management
- 458 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Distal Radius Fractures
Evidence-Based Management
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
OrthopedicsSection IV
Acute Fracture Management
Chapter 7: Closed Reduction and Immobilization of Displaced Distal Radius Fractures
Hyoung-Seok Jung; Jae-Sung Lee Department of Orthopedic Surgery, Hospital of Chung-Ang University of Medicine, Seoul, Republic of Korea
Abstract
Despite the popularity of surgical treatment, most displaced distal radius fractures (DRFs) are initially managed with closed reduction and immobilization. What is the most effective technique for closed reduction and immobilization in the treatment of DRFs? Here, we tried to describe the optimal methods based on the evidence. In terms of the reduction technique, hematoma block is able to be recommendable, while reduction using finger-trap traction does not seem to be effective comparing manual reduction. Immobilization with a sugar tong or above-the-elbow splint is equivalent to a short-arm splint for maintaining the reduction. The evidence of the benefit of repeating reduction in DRFs is insufficient.
Keywords
Close reduction; Immobilization; Displaced distal radius fracture
Key Points
- • Despite the popularity of surgical treatment, most displaced distal radius fractures (DRFs) are initially managed with closed reduction and immobilization.
- • Radiological outcomes were not significantly different between mechanical reduction using finger-trap traction and manual reduction.
- • Compared to procedural sedation, local anesthesia (hematoma block) is a safe and effective alternative anesthesia for reduction of DRFs, which provides excellent pain relief in adult and pediatric patients.
- • Immobilization using a sugar-tong or above-the-elbow splint is equivalent to a short-arm splint for maintaining the reduction and quality of molding has more influence on maintaining reduction than the length of the cast.
- • The evidence of the benefit of routinely repeating reduction or routine preoperative reduction in DRFs is insufficient
- • Repeated reduction should be reserved for experienced teams in selected patients, such as those with minimal comminution, those who fail to get appropriate reduction due to inadequate anesthesia or those who have relative contraindications to surgery.
Panel 1: Case Scenario
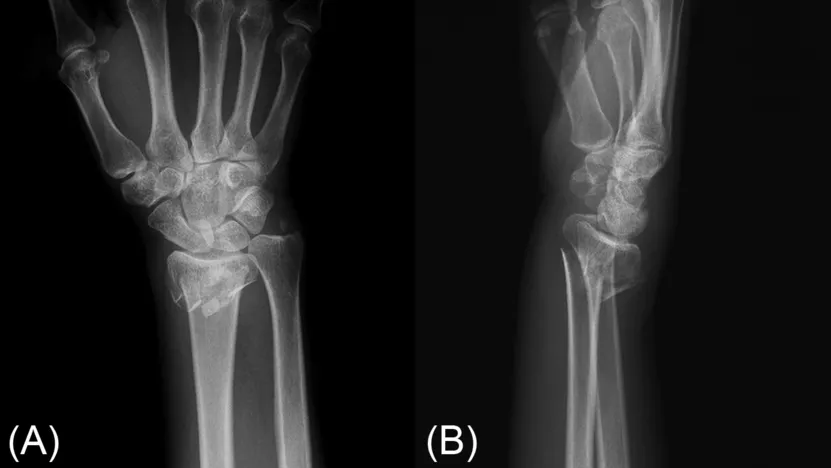
A 46-year-postmenopausal woman visited the emergency department with a swollen and deformed right wrist after falling on an outstretched hand. Radiographs showed a displaced distal radius fracture with a 40 degrees dorsal angulation and metaphyseal comminution (Fig. 1). How is her fracture most effectively reduced and maintained?
Importance of the Problem
Distal radius fractures (DRFs) are a common orthopedic condition among adults and high incidence is reported worldwide.1–3 Multiple treatment options are available for patients with DRFs, including cast immobilization, percutaneous pinning, external fixation, and open reduction with internal fixation (ORIF) using a plate. The optimal choice depends on several factors such as patient age, fracture pattern, displacement, fracture instability, and surgeon preference. Over the recent decades, surgical approaches such as ORIF have been increasingly used.2, 4, 5 Despite the popularity of ORIF, most displaced DRFs are initially managed with closed reduction and subsequent orthosis. Closed reduction of DRFs is commonly performed in the emergency department to obtain acceptable fracture alignment and maintain stability. In some cases, two or more reduction attempts are performed to achieve these goals.6
Main Question
What is the most effective technique for closed reduction and immobilization in the treatment of DRFs?
Current Opinion
The initial management of DRFs typically consists of closed reduction and immobilization in the emergency department. The quality of reduction can influence definitive management; thus, some authors have suggested that significant efforts should be made to obtain anatomical reduction when possible. Therefore, a combination of closed reduction and cast immobilization remains a preferred treatment option in most cases. However, the optimal method for closed reduction remains to be determined.
Closed reduction of a fracture is considered acceptable when the following radiologic conditions are obtained: radial inclination ≥ 15 degrees, loss of radial height ≤ 5 mm, dorsal angulation ≤ 15 degrees and palmar angulation ≤ 20 degrees.7 The classic method of closed reduction for DRFs requires two people pulling in opposite directions to produce and maintain longitudinal traction. This is termed manual reduction. The mechanical methods of reduction usually include the use of “finger traps.” In fi...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- Dedication
- Section Editors
- Contributing Authors
- Preface
- Section I: Introduction
- Section II: Anatomy and Biomechanics
- Section III: Diagnostic Management
- Section IV: Acute Fracture Management
- Section V: Pediatric Fracture Management
- Section VI: Elderly Fracture Management
- Section VII: Malunion and Nonunion
- Section VIII: Posttraumatic Arthritis and Complications
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Distal Radius Fractures by Geert Alexander Buijze,Jesse Jupiter,Michel Chammas,Geert Buijze, Geert Buijze, Jesse Jupiter, Michel Chammas in PDF and/or ePUB format, as well as other popular books in Medicine & Orthopedics. We have over 1.5 million books available in our catalogue for you to explore.