Flavio Andres Uribe, Taranpreet K. Chandhoke, Ravindra Nanda
The term diagnosis is defined as the identification of a disease by careful investigation of its symptoms and history.1 While not a true disease per se, malocclusions are the “disease” processes of orthodontics and the central focus of orthodontic diagnoses. Malocclusions can have esthetic and functional implications, and an accurate diagnosis is required to best understand their etiology and the treatment options for managing the abnormality. From an esthetic standpoint, there are psychological implications associated with malocclusions related to social acceptance and success.2 From a functional standpoint, mastication, speech, and protection of the structures in the entire stomatognathic system can contribute to or be the result of the malocclusion that is present.
To define the abnormal or pathological characteristics of the malocclusion, there needs to be an appreciation of what is defined as “normal.” This is a particular challenge because what is considered normal falls within a wide range. Variability is found throughout nature, so defining the limits of the normal range can be difficult. While esthetic perceptions vary through history and among individuals, races, and cultures, ideal occlusion and its functional implications are characterized by strict morphological features. Thus the definition of a normal occlusion involves both objective and subjective components.
Extensive research has determined the characteristics of normal functional occlusion. Concepts such as cusp-to-fossa or cusp-to-interproximal space occlusion, lateral and anterior guidance, and mutually protected occlusion are described comprehensively in other textbooks.3 However, the criteria for ideal occlusal function are better defined in comparison to ideal esthetic values. Most of the occlusal concepts accepted today are derived from the assumed premise that good anatomy (i.e., good occlusal interdigitation) is analogous to proper function (Fig. 1-1).
Figure 1-1 A–C, Frontal and lateral views of an ideal occlusion.
From the esthetic standpoint, orthodontists base their judgment on cephalometric norms obtained many decades ago from population samples with vaguely defined parameters of esthetics. In general, these studies assumed that good occlusion was directly related to good facial esthetics. Although these measurements provide some objective guidelines that can be used to start defining how each patient differs from the norm, there are limitations to these analyses. Furthermore, it is not the absolute numeric amounts and their variation that dictate treatment but the accurate interpretation of these and all data obtained from the clinical examination and other patient records.
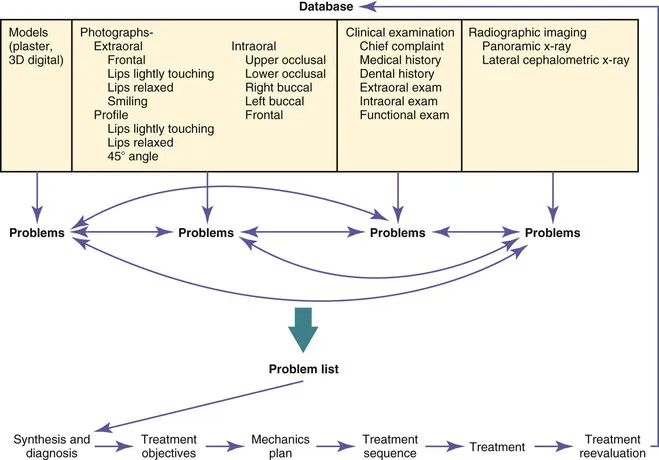
To accurately diagnose a malocclusion, orthodontics has adopted the problem-based approach originally developed in medicine.4 Every factor that potentially contributes to the etiology, might contribute to the abnormality, or might influence treatment should be evaluated. Information is gathered through a medical and dental history, clinical examination, and records that include models, photographs, and radiographic imaging. A problem list is generated from the analysis of the database that contains a network of interrelated factors. The diagnosis is established after a continuous feedback between the problem recognition and the database. Ultimately, the diagnosis should provide some insight into the etiology of the malocclusion (Fig. 1-2).
Figure 1-2 Steps in diagnosis and treatment planning.
The diagnosis and problem list is the framework that dictates the treatment objectives for the patient. Once formulated, the treatment plan is designed to address those objectives, from the mechanics to the sequence that will be used.
From the treatment objectives perspective, one or more treatment options can be developed to address each objective. Each treatment option will have advantages and disadvantages for the patient. During the process of obtaining informed consent from the patient, clear descriptions of the advantages, disadvantages, and risks of each treatment plan should be presented and the patient will ultimately determine the final treatment plan. The treatment plan then dictates the mechanics plan designed to achieve the desired goals with the greatest efficiency and fewest side effects.
This chapter discusses some of the objective measures that define the range of normality, both from an occlusal and a dentofacial standpoint. It is important to know that although emphasis is placed on the entire dentofacial complex, there are limits to the amount of correction that can be achieved with orthodontic treatment.
The clinician has to work within certain constraints and understand the limitations of the various treatment options. For example, the soft tissue envelope allows for only a certain amount of correction. If major movements are needed, they may require other treatment options such as surgery or skeletal anchorage, which, although able to achieve a wider range of movements, are limited by the boundaries of the soft tissue envelope. The primary goal should be to achieve the best possible facial balance and functional occlusion.
Finally, while great care is taken in formulating a detailed treatment plan, it is important to realize that the diagnosis and treatment plan are dynamic processes. As the plan is executed, continuous monitoring and effective evaluation of the objectives are needed. Appropriate reassessment, adjustment, and corrective measures to the original plan are crucial if all specific goals and not only the occlusal goals are to be achieved.
As described above, very precise collection of data is needed to achieve a proper diagnosis. The database should include a thorough medical and dental history, a set of models, the necessary radiographs, and a clinical examination accompanied by extraoral and intraoral photographs.
Clinical Examination
Medical and Dental History
“What is the patient's chief complaint?” This question is the basis of the anamnesis. At a minimum, the treatment plan should aim to address this important fundamental component of the patient's initial screening. The clinician is responsible for accurately understanding and addressing the chief complaint. Some patients will have very specific ...