Vertigo and Imbalance: Clinical Neurophysiology of the Vestibular System
eBook - ePub
Vertigo and Imbalance: Clinical Neurophysiology of the Vestibular System
Handbook of Clinical Neurophysiology
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Vertigo and Imbalance: Clinical Neurophysiology of the Vestibular System
Handbook of Clinical Neurophysiology
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Chapter 1
Overview of vestibular and balance disorders
Scott D.Z. Eggersa* and David S. Zeeb, aDepartment of Neurology, Mayo Clinic College of Medicine, 200 First St. SW, Rochester, MN 55905, USA; bDepartment of Neurology, The Johns Hopkins Hospital, Path 2-210, 600 N. Wolfe St., Baltimore, MD 21287, USA. E-mail address: [email protected]
*Correspondence to: Dr. Scott D.Z. Eggers, Department of Neurology, Mayo Clinic College of Medicine, 200 First St. SW, Rochester, MN 55905, USA. (S.D.Z. Eggers)
Publisher Summary
This chapter reviews the basic vestibular and ocular motor anatomy, and physiology relevant to patients with balance disorders. Then with a foundation of physiological and anatomical principles in mind, the historical features and special bedside examination techniques for evaluating the dizzy patient are discussed. It explores that great advances have been made in the past half century in the ability to study and quantify the characteristics of eye movements, and the influence of the vestibular and optokinetic systems on ocular motor control. This, combined with careful clinical observation of patients, has led to the discovery of new disorders, such as superior canal dehiscence and treatments like the canalith repositioning procedure. The chapter also reviews that rational model of the neural basis for vestibular and ocular motor control can be created, and tested experimentally with great precision.
This volume of the Clinical Neurophysiology Handbook Series is devoted to the clinical neurophysiology of vestibular and balance disorders. This large subject is covered by 40 chapters written by experts from around the world. As Editors of the volume, we are indebted to these authors for their unselfish dedication and far-reaching contributions.
Clinicians and scientists involved in the research and care of patients with dizziness are defined not by an anatomic specialty or disease, but rather by the nature of their patients’ presenting complaints: vertigo, disequilibrium, imbalance, and related symptoms. Thus, the target audience for this volume is reflected in the diverse backgrounds of its authors — neurologists, otolaryngologists, neuro-ophthalmologists, audiologists, physical therapists, psychiatrists, and bioengineers. Indeed a multidisciplinary approach is essential for the optimal diagnosis and treatment of patients with vestibular disorders. The goal of this volume is to review each topic with enough background to be accessible to the non-specialist, while at the same time providing depth and completeness for the specialist and methodological detail for the clinician, technician, or investigator.
This volume has been divided into four major sections:
(1) The Overview section reviews basic vestibular and ocular motor anatomy and physiology relevant to patients with balance disorders. Then with a foundation of physiological and anatomical principles in mind, the historical features and special bedside examination techniques for evaluating the dizzy patient are discussed.
(2) The Methodological Techniques section reviews in depth the great breadth of techniques now available to evaluate the function of the vestibular system. Beginning with the various techniques of recording eye movements, this section covers standard methods such as rotary chair testing and caloric testing, as well as recently developed or specialized tests such as head impulse testing, translational vestibulo-ocular reflex testing, vestibular evoked potentials, electrocochleography, and provocative maneuvers. Many of these emerging techniques have not been previously reviewed systematically. Many have not reached widespread clinical use but are in development or are useful research tools. Methodological descriptions are not repeated later in the chapters covering specific diseases, so the reader will need to refer back to these chapters for description of techniques and normal values.
(3) Chapters in the Diseases and Treatments section address the most common conditions and important issues relevant to care of patients with vestibular and balance disorders. Topics range from peripheral vestibular disorders to neurological disorders, with additional discussion of psychological issues, visual symptoms, and the elderly. Both “new” diagnoses (e.g., migrainous vertigo and superior canal dehiscence) and more traditional causes of vestibular dysfunction (e.g., Ménière’s disease and vestibular neuritis) are discussed. Given the focus of this volume and series, special attention is paid to the role of available testing techniques in the diagnosis and management of patients.
(4) A final chapter looks back at the historical roots of the study of vestibular and ocular motor function. Based upon our expanding fundamental understanding and computational modeling of these systems, the authors look ahead to the next decade for methodological approaches and advances, such as use of artificial neural networks to aid diagnosis, development of vestibular prostheses, study of the perceptual disturbances often reported by patients with vestibular dysfunction, and finally treatment approaches based upon the molecular biology and genetics of vestibular disease.
Evaluating dizzy patients with vertigo and other “spells” of symptoms requires some knowledge in several areas, including cardiovascular and autonomic disorders, psychiatry, and areas within neurology such as cerebrovascular disease, epilepsy, and migraine. Readers may need to consult other textbooks for further details on cardiovascular diseases, autonomic disorders, and epilepsy, all of which can sometimes lead to dizziness and falls.
Great advances have been made in the past half century in the ability to study and quantify the characteristics of eye movements and the influence of the vestibular and optokinetic systems on ocular motor control. This, combined with careful clinical observation of patients, has led to the discovery of new disorders such as superior canal dehiscence and treatments such as the canalith repositioning procedure. Rational models of the neural basis for vestibular and ocular motor control can be created and tested experimentally with great precision. Yet clinical care of patients with dizziness and vertigo is still often empiric and messy. Many important basic and clinical questions remain unanswered. What is the underlying pathophysiological basis for Ménière’s syndrome and migrainous vertigo, and how are they related? How can we promote regeneration or engineer alternatives in the setting of vestibular damage? Can pharmacogenetics be applied for the rational treatment of vestibular disorders?
The field is ripe for further research. Collaboration is needed among clinicians, basic scientists, engineers, radiologists, molecular biologists, and geneticists. We hope that this book will provide a framework for basic knowledge and inspiration for further study.
Chapter 2
Overview of anatomy and physiology of the vestibular system
Terry D. Fife*, Department of Neurology, University of Arizona College of Medicine, and Arizona Balance Center, Barrow Neurological Institute, Phoenix, AZ 85013, USA. E-mail address: [email protected]
*Correspondence to: Terry D. Fife, Arizona Balance Center, Barrow Neurological Institute, 222 W. Thomas Road, Suite 110A, Phoenix, AZ 85013, USA. Tel.: +1-602-406-6338; fax: +1-602-406-6339.
Publisher Summary
This chapter reviews that the vestibular system helps to maintain spatial orientation and stabilize vision for the purpose of maintaining balance, especially during movement. Vestibular end organs sense angular and linear acceleration, and transduce these forces to electrochemical signals that can be used by the central nervous system. It discusses that the central nervous system integrates the information from the vestibular system to stabilize gaze during head motion by means of the vestibulo-ocular reflex (VOR) and to modulate muscle tone by the vestibulocollic and vestibulospinal reflexes. The vestibular system detects angular and linear acceleration through five end organs of the membranous labyrinth on each side: the saccule; the utricle; and the anterior, posterior, and lateral semicircular canals. The saccule and the utricle, the otolith organs, transduce linear accelerations, be they from the pull of gravity or from translation of the head. Each of the semicircular canals has a different spatial orientation; the summation of signals from the semicircular canals allows one to detect rotation of the head in any direction.
2.1 Introduction
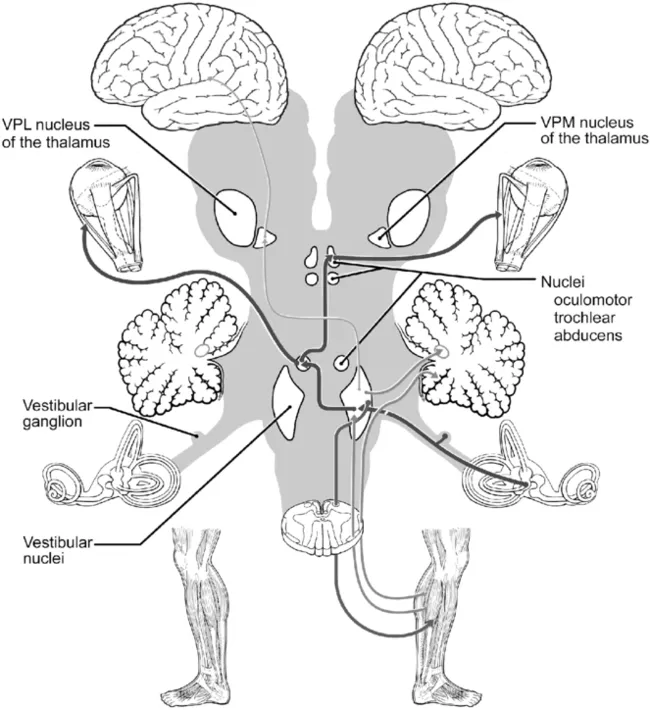
The vestibular system helps to maintain spatial orientation and stabilize vision for the purpose of maintaining balance, especially during movement. Vestibular end organs sense angular and linear acceleration and transduce these forces to electrochemical signals that can be used by the central nervous system. The central nervous system integrates the information from the vestibular system to stabilize gaze during head motion by means of the vestibulo-ocular reflex (VOR) and to modulate muscle tone by the vestibulocollic and vestibulospinal reflexes (Fig. 1).
The vestibular system detects angular and linear acceleration through five end organs of the membranous labyrinth on each side: the saccule, the utricle, and the anterior, posterior and lateral semicircular canals (Fig. 2). The saccule and utricle, the otolith organs, transduce linear accelerations, be they from the pull of gravity or from translation of the head. Each of the semicircular canals has a different spatial orientation; the summation of signals from the semicircular canals allows one to detect rotation of the h...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright page
- Dedication
- Foreword
- List of Contributors
- Chapter 1: Overview of vestibular and balance disorders
- Chapter 2: Overview of anatomy and physiology of the vestibular system
- Chapter 3: Overview of anatomy and physiology of the ocular motor system
- Chapter 4: Bedside assessment of the dizzy patient
- Chapter 5: Eye movement measurement
- Chapter 6: Magnetic scleral search coil
- Chapter 7: Ocular motor testing techniques and interpretation
- Chapter 8: Positioning and positional nystagmus testing
- Chapter 9: Provocative maneuvers for vestibular disorders
- Chapter 10: Caloric testing
- Chapter 11: Rotational testing
- Chapter 12: Head impulse testing
- Chapter 13: Vestibulo-ocular responses to sound, vibration and galvanic stimulation
- Chapter 14: Computerized dynamic visual acuity test in the assessment of vestibular deficits
- Chapter 15: Vestibular-evoked myogenic potentials (VEMPs)
- Chapter 16: Otolith testing
- Chapter 17: Otolith testing
- Chapter 18: The cervico-ocular reflex
- Chapter 19: Computerized postural control assessment1
- Chapter 20: Evaluation of gait and turns
- Chapter 21: Auditory function in the dizzy patient
- Chapter 22: Electrocochleography
- Chapter 23: Brainstem auditory evoked potentials (BAEPs) and intraoperative BAEP monitoring
- Chapter 24: Functional brain imaging of the vestibular system
- Chapter 25: Vestibular neuritis
- Chapter 26: Acquired bilateral peripheral vestibulopathy
- Chapter 27: Benign paroxysmal positional vertigo
- Chapter 28: Ménière’s disease
- Chapter 29: Temporal bone and cerebellopontine angle tumors
- Chapter 30: Superior semicircular canal dehiscence syndrome and perilymphatic fistula
- Chapter 31: Autoimmune inner ear disease
- Chapter 32: Inherited vestibular and vestibulocerebellar disorders
- Chapter 33: Migrainous vertigo
- Chapter 34: Vestibular disorders in cerebrovascular disease
- Chapter 35: Vestibular testing and multiple sclerosis
- Chapter 36: Post-traumatic dizziness
- Chapter 37: Dizziness in older people
- Chapter 38: Psychological aspects of vestibular disorders
- Chapter 39: Visual symptoms and vertigo
- Chapter 40: Vestibular and ocular motor function
- Subject Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Vertigo and Imbalance: Clinical Neurophysiology of the Vestibular System by S. D. Eggers,D. Zee, S. D. Eggers, D. Zee in PDF and/or ePUB format, as well as other popular books in Medicine & Neurology. We have over 1.5 million books available in our catalogue for you to explore.