Sleep Medicine is a rapidly growing and changing field. Experienced sleep medicine clinicians and educators Richard B. Berry, MD and Mary H. Wagner, MD present the completely revised, third edition of Sleep Medicine Pearls featuring 150 cases that review key elements in the evaluation and management of a wide variety of sleep disorders. The cases are preceded by short fundamentals chapters that present enough basic information so that a physician new to sleep medicine can start reading page 1 and quickly learn the essential information needed to care for patients with sleep disorders. A concise, practical format makes this an ideal resource for sleep medicine physicians in active practice, sleep fellows learning sleep medicine, and physicians studying for the sleep boards.- Consult this title on your favorite e-reader, conduct rapid searches, and adjust font sizes for optimal readability.- Zero in on the practical, "case-based" information you need to effectively interpret sleep studies (polysomnography, home sleep testing, multiple sleep latency testing), sleep logs, and actigraphy.- Get clear, visual guidance with numerous figures and sleep tracings illustrating important concepts that teach the reader how to recognize important patterns needed to diagnose sleep disorders.- Confer on the go with short, templated chapters—ideal for use by busy physicians. A combination of brief didactic material followed by case-based examples illustrates major points.- Stay current with knowledge about the latest developments in sleep medicine by reading updated chapters using the new diagnostic criteria of the recently published International Classification of Sleep Disorder, 3rd Edition and sleep staging and respiratory event scoring using updated versions of the scoring manual of the American Academy of Sleep Medicine Manual for the Scoring of Sleep and Associated Events.- Benefit from Drs. Berry and Wagner's 25+ years of clinical experience providing care for patients with sleep disorders and educational expertise from presenting lectures at local, regional and national sleep medicine courses. Dr Berry was awarded the AASM Excellence in Education Award in 2010.- Access the full contents online at ExpertConsult.
- 580 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Sleep Medicine Pearls E-Book
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
Ear, Nose & Throat MedicineFundamentals 1
Sleep Stage Nomenclature and Basic Monitoring of Sleep
Introduction
Sleep is divided into non–rapid eye movement (NREM) and rapid eye movement (REM) sleep. From 1968 until 2007, sleep was usually staged according to A Manual of Standardized Terminology, Techniques, and Scoring System for Sleep Stages of Human Subjects, edited by Rechtschaffen and Kales (R&K).1 In the R&K Scoring Manual, NREM sleep was divided in stages 1, 2, 3, and 4. REM sleep was referred to as stage REM. Sleep stage nomenclature has changed following the publication of the American Academy of Sleep Medicine (AASM) Manual for the Scoring of Sleep and Associated Events (hereafter referred to as the AASM Scoring Manual) in 2007.2,3 To denote sleep staging by new criteria, sleep stage nomenclature has changed. The old and new nomenclatures are shown in Table F1-1. Stages 3 and stage 4 are combined into stage N3. REM sleep is referred as stage R. An update of the AASM Scoring Manual has recently been published, but sleep stage nomenclature remains unchanged.4
Table F1-1
Sleep Stage Nomenclature
| R&K | AASM | |
| Wake | Stage W | Stage W |
| NREM | Stage 1 | Stage N1 |
| Stage 2 | Stage N2 | |
| Stage 3 | Stage N3 | |
| Stage 4 | ||
| REM | Stage REM | Stage R |
AASM, American Academy of Sleep Medicine; NREM, non–rapid eye movement; REM, rapid eye movement; R&K, Rechtschaffen and Kales.
Sleep staging is based on electroencephalography (EEG), electrooculography (EOG), and submental (chin) electromyography (EMG) criteria. EOG (eye movement recording) and chin EMG recordings are used to detect stage R, which is characterized by rapid eye movements (REMs) and reduced muscle tone.
Time Window for Staging Sleep
Digital polysomnography (sleep recording) allows visualization of the waveforms in multiple time windows (10, 15, 30, 60, 90, 120, and 240 seconds) (Table F1-2). A 30-second window is used to stage sleep (known as an epoch), whereas a 10-second window is used for clinical electroencephalography (EEG) monitoring. A 10-second window allows for detailed visualization of waveforms to determine frequency. The convention of using a 30-second window for sleep staging is based on paper recording using ink pens during the early days of sleep monitoring. At a page speed of 10 millimeters per second (mm/s), a standard 30-centimeter (cm) page of recording paper represented 30 seconds. Each page represented one epoch. Sleep is still staged today in sequential 30-second epochs, although digital polysomnography allows for use of different time windows for scoring respiratory and other events.
Table F1-2
Optimal Window Duration for Viewing Events in Polysomnography
| Window Duration | Use |
| 30 seconds (an epoch) | Sleep staging |
| 60–120 seconds | Respiratory Events |
| 15 seconds | Clinical EEG |
| 10 seconds | ECG rhythms Identifying wave form frequency |
ECG, Electrocardiography; EEG, electroencephalography.
Electroencephalography Monitoring
EEG monitoring to detect and stage sleep requires only a portion of the electrodes used for clinical EEG monitoring. The nomenclature for EEG electrodes follows the International 10-20 system.5 In this system, even-numbered subscripts refer to the right side of the head and odd-numbered subscripts to the left. Electrodes are named for the part of the brain they cover: F for frontal, C for central, and O for occipital (Figure F1-1). The central midline (vertex) electrodes (Cz) and the frontopolar midline electrode (Fpz) are also of interest. The Fpz position is often used for the ground electrode and the Cz position for the reference electrode. Note that before publication of the AASM Scoring Manual, electrodes M1 and M2 were referred to as A1 and A2, respectively. In clinical EEG monitoring, A1 and A2 are, in fact, referred to as earlobe electrodes.
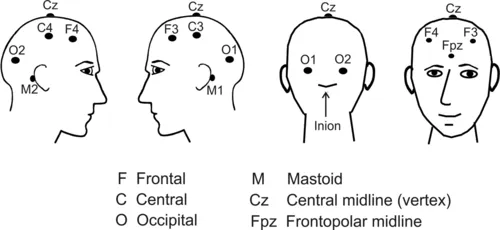
Figure F1-1 Nomenclature and position of the basic electrodes for sleep monitoring. C, Central; F, frontal; O, occipital. Even numbers on the right and odd on the left. (Adapted from Berry RB: Fundamentals of sleep medicine, Philadelphia, 2012, Saunders, pp. 2-3.)
The “10-20” in the International 10-20 system of nomenclature for EEG electrodes refers to the fact that the electrodes are positioned at either 10% or 20% of the distance between landmarks.5 The major landmarks include the nasion (bridge of the nose), inion (prominence at base of the occiput), and preauricular points (Figure F1-2).
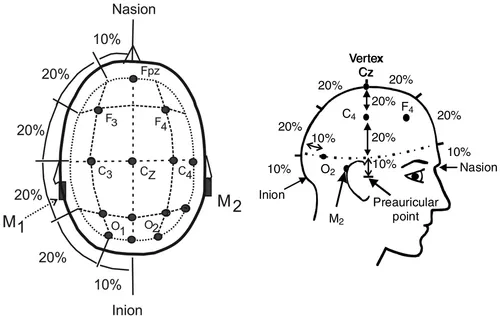
Figure F1-2 Electrode positions using the international 10-20 system. Electrodes are placed at 10% or 20% of the distance between landmarks. (Adapted from Berry RB: Fundamentals of sleep medicine, Philadelphia, 2012, Saunders, pp. 2-3.)
Electroencephalography Derivations
EEG recording uses differential alternating current (AC) amplifiers, which are designed to amplify the difference in voltage between electrodes. There is cancellation of signals common to both electrodes (common mode rejection). (Figure F1-3), this type of AC amplifier allows the recording of relatively low-voltage EEG activity superimposed on a background of high...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- Dedication
- Preface
- Video Contents
- Fundamentals 1: Sleep Stage Nomenclature and Basic Monitoring of Sleep
- Fundamentals 2: Electroencephalography and Electrooculography Patterns of Interest for Staging Sleep
- Fundamentals 3: Sleep Staging in Adults I
- Fundamentals 4: Scoring Stage R
- Fundamentals 5: Arousals and Major Body Movements
- Fundamentals 6: Sleep Staging in Infants and Children
- Fundamentals 7: Sleep Architecture Terminology and Normal Patterns
- Fundamentals 8: Effects of Sleep Disorders and Medications on Sleep Architecture
- Fundamentals 9: Polysomnography I
- Fundamentals 10: Indications for Polysomnography, Portable Monitoring, and Actigraphy
- Fundamentals 11: Artifacts
- Fundamentals 12: Monitoring Respiration
- Fundamentals 13: Respiratory Event Definitions in Adults
- Fundamentals 14: Respiratory Events in Children
- Fundamentals 15: Electrocardiography Monitoring During Sleep Studies
- Fundamentals 16: Monitoring Limb and Other Movements During Sleep
- Fundamentals 17: Subjective and Objective Measures of Sleepiness
- Fundamentals 18: Sleepiness and Sleep Complaints in Children
- Fundamentals 19: Diagnosis of Obstructive Sleep Apnea Syndromes in Adults
- Fundamentals 20: Obstructive Sleep Apnea in Adults: Epidemiology and Variants
- Fundamentals 21: Pediatric Obstructive Sleep Apnea
- Fundamentals 22: Obstructive Sleep Apnea: Treatment Overview and Medical Treatments
- Fundamentals 23: PAP Modes and Treatment
- Fundamentals 24: PAP Titration and Auto-Titration
- Fundamentals 25: PAP Adherence
- Fundamentals 26: Surgical Treatment for Obstructive Sleep Apnea
- Fundamentals 27: Oral Appliance Treatment for Obstructive Sleep Apnea
- Fundamentals 28: Asthma and COPD
- Fundamentals 29: Central Sleep Apnea and Sleep-Related Hypoventilation Disorders
- Fundamentals 30: Advanced PAP Modes and NPPV Titration
- Fundamentals 31: Diagnosis of RLS and PLMD
- Fundamentals 32: Treatment of RLS and PLMD
- Fundamentals 33: Hypersomnolence of Central Origin-I
- Fundamentals 34: Hypersomnolence of Central Origin II
- Fundamentals 35: Parasomnia
- Fundamentals 36: Clinical Electroencephalography and Epilepsy
- Fundamentals 37: Evaluation of Insomnia
- Fundamentals 38: Behavioral Treatment of Insomnia
- Fundamentals 39: Pharmacologic Treatment of Insomnia
- Fundamentals 40: Circadian Rhythm Sleep-Wake Disorders
- Fundamentals 41: Psychiatry and Sleep
- Appendix 1: Normal Ranges for Sleep Architecture
- Appendix 2: Typical Values for Sleep Parameters in Normal Children
- Appendix 3: Medicare Guidelines for Reimbursement for Respiratory Assist Device
- Glossary
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Sleep Medicine Pearls E-Book by Richard B. Berry,Mary H. Wagner,Mary H Wagner in PDF and/or ePUB format, as well as other popular books in Medicine & Ear, Nose & Throat Medicine. We have over 1.5 million books available in our catalogue for you to explore.