As proton therapy treatment centers become smaller and more cost-effective, education and training for today's multi-disciplinary oncology teams are more important than ever before. This state-of-the-art reference brings you fully up to date with all aspects of proton therapy, with guidance you can trust from MD Anderson Cancer Center, the largest and most experienced proton therapy center in the world. Led by Drs. Steven J. Frank and W. Ronald Zhu, Proton Therapy provides a unique opportunity to benefit from the unsurpassed knowledge and expertise of an esteemed team of leaders in the field.
- Covers all cancers for which proton therapy is used most often, including prostate, head and neck, pediatrics, central nervous system, gastrointestinal, sarcomas, lungs, breast, lymphomas, and gynecologic cancers.
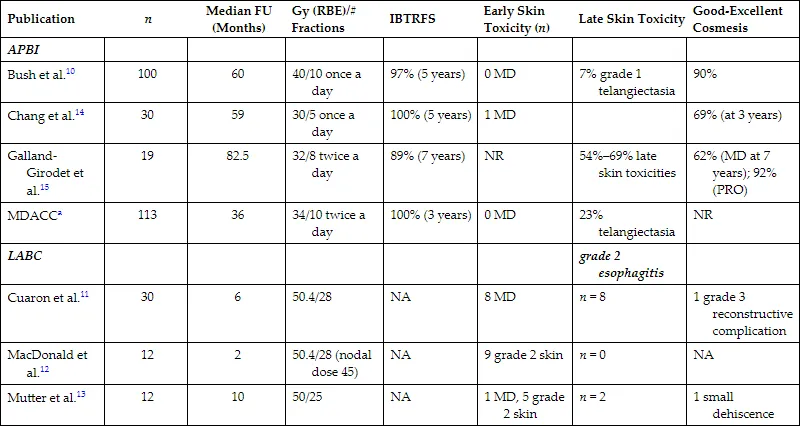
- Provides up-to-date information on radiobiology, treatment planning and quality assurance, indications for proton therapy, management approaches, and outcomes after proton therapy by disease site.
- Discusses technologic advances such as spot scanning and treatment planning systems for the management of solid tumors; radiobiology of proton therapy, including DNA damage and repair mechanisms and acute and late effects on normal tissues; and multifield optimized intensity-modulated proton therapy (MFO-IMPT) for optimizing the distribution of linear energy transfer (LET) of proton beams within target volumes and away from critical normal structures.
- Includes a special section on head and neck cases in the e-book that photographically illustrates the full cycle of proton therapy care.