Children and infants comprise up to 20% of emergency department visits, and emergency physicians must be knowledgeable in choosing the most appropriate imaging modality to arrive at an accurate diagnosis and provide optimal patient care. Written specifically for the non-specialist and those with limited pediatric training, Pediatric Imaging for the Emergency Provider provides expert guidance in this challenging area. Abundant high-quality imaging examples cover the full range of pediatric disorders you're likely to see, including trauma, musculoskeletal, pulmonary, ENT, cardiac, genitourinary, gastroenterology, neurological, and neonatal patients.- Presents more than 80 common and important rare cases, supported with 450+ images across relevant modalities including ultrasound, radiography, CT, and MRI.- Identifies key radiographic findings for various pediatric conditions including congenital heart lesions, surgical entities, infectious disease processes, and traumatic injuries.- Accompanies images with clear, concise text that makes it easy to grasp the most clinically significant points of each case.- Provides expert guidance on best practices in important areas of pediatric imaging such as sedation, ionizing radiation exposure reduction, and imaging modality selection.
eBook - ePub
Pediatric Imaging for the Emergency Provider E-Book
- 400 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Pediatric Imaging for the Emergency Provider E-Book
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
Medicine SECTION 1
Neonatal
Outline
- 4. My, what a big thymus you have! Neonate/infant mediastinal masses
- 5. A wheezin’ we will go: Bronchiolitis/viral pathology
- 6. Twisting the night away: Malrotation
- 7. Double bubble. . . double trouble! Duodenal obstruction
- 8. Cyanotic and acyanotic congenital heart disease
- 9. More than constipation: Failure to pass meconium
- 10. Rumbly in the tumbly: Pneumatosis intestinalis and necrotizing enterocolitis
4: My, what a big thymus you have! Neonate/infant mediastinal masses
Robert Vezzetti, MD, FAAP, FACEP
Case presentation
An 8-month-old male presents with 2 months of cough and intermittent rhinorrhea. He has been seen multiple times by his primary care provider and has been diagnosed at various times with viral upper respiratory tract infection and acute otitis media, for which he has been prescribed oral antibiotics. He has had some intermittent fevers as well, all of which have resolved after several days. There has been no travel or sick contacts, nor has there been any history of choking or concern for foreign body ingestion.
Physical examination reveals a thin but well-appearing and active child. He is afebrile and his vital signs are unremarkable, except for mild tachypnea (65 breaths per minute). There is no rhinorrhea and the oropharynx is clear. His chest demonstrates decreased breath sounds to the upper left chest, but there are no crackles, retractions, grunting, or stridor. He has a normal abdominal examination.
Imaging considerations
Plain radiography
This imaging modality is the most commonly utilized imaging modality for the neonatal or infant chest.1 Two views are preferred (anterior-posterior [AP] and lateral) when possible. Plain radiography may suggest the presence of a chest mass, prompting the use of advanced imaging. Ninety percent of chest masses can be visualized by plain radiography.2
Plain radiography is the first-line imaging modality when chest masses are suspected.3 However, this modality may miss small masses, and further imaging is indicated when a mediastinal mass is suspected, since a diagnosis is not usually made by plain radiography alone.3
Ultrasound (US)
This imaging modality is increasingly used for the evaluation of specific chest conditions. Examples include pneumothorax, pleural effusion, hemothorax, and chest masses.1 US of the mediastinum is limited, however, in patients above 5 years of age due to poor acoustic windows.3 The lack of exposure to ionizing radiation, rapidity, availability, and no need for sedation are all advantages of sonography.
Computed tomography (CT)
This imaging modality is typically utilized when plain radiography is abnormal and further delineation of a suspected chest mass is indicated. CT is also used for surgical planning when indicated.1 CT is readily available and rapid and usually does not require sedation. CT does include exposure to ionizing radiation, and appropriate pediatric imaging protocols should be utilized to reduce this exposure as much as possible.
CT is often utilized in patients with mediastinal masses. It has been shown to be very accurate for the characterization of masses (such as size and location) and to determine whether there is involvement of adjacent structures.2–4 CT can differentiate between cystic and solid structures and can evaluate for the presence of calcification, fat, or vascular components.2 CT findings have been shown to impact management in 65% of cases and have added additional diagnostic information in 82%.3,4
Magnetic resonance imaging (MRI)
As with CT, MRI is used for further anatomic definition and tissue characterization of suspected chest masses. MRI is particularly good at differentiating cystic from solid structures, especially compared to CT.2,3 MRI may also be used when planning surgical procedures.1 Availability and the need for sedation are potential disadvantages of MRI.
Positron emission tomography (PET)
PET is not a first-line imaging modality for diagnosing mediastinal masses in pediatric patients. However, PET imaging, including PET-CT or PET-MRI, can be used in staging tumors and monitoring response to therapy.3,5 Such imaging for children, though, is usually found at tertiary pediatric centers and generally is not widely available.
Imaging findings
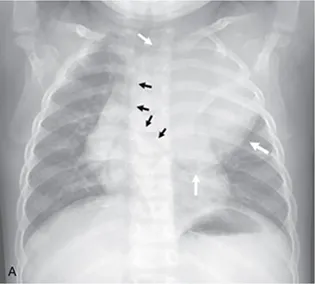
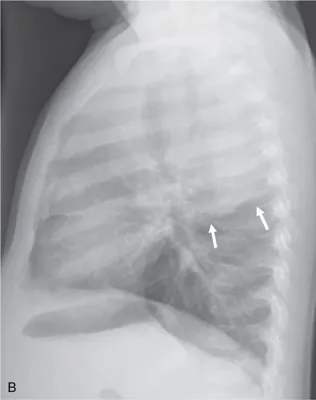
The patient had two-view plain radiography of the chest performed. There is a large rounded opacity in the left mid to upper chest that has a well-defined border laterally and inferiorly. There is mass effect on the lower trachea (displacement to the right) and left mainstem bronchus (displaced inferiorly and medially) (Fig. 4.1).
Case conclusion
The patient was admitted with consultation by Pediatric Oncology and Pediatric Surgery. A contrast-enhanced CT scan of the chest was obtained, demonstrating the mass, which appears centered in the posterior left mediastinum but extends to involve the middle and anterior mediastinum (Fig. 4.2). CT-guided biopsy revealed that ...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- Dedication
- List of contributors
- Preface
- Acknowledgement
- List of Tables
- List of Illustrations
- Introduction
- Section 1. Neonatal
- Section 2. Cardiac
- Section 3. Gastroenterology
- Section 4. Genitourinary
- Section 5. Neurologic
- Section 6. Pulmonary
- Section 7. Trauma
- Section 8. Musculoskeletal
- Section 9. ENT
- Appendix 1: Imaging pathways
- Appendix 2: Imaging acronyms
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Pediatric Imaging for the Emergency Provider E-Book by Robert Vezzetti,Jestin Carlson,Debra Pennington, Robert Vezzetti, Jestin Carlson, Debra Pennington in PDF and/or ePUB format, as well as other popular books in Medicine & Emergency Medicine & Critical Care. We have over 1.5 million books available in our catalogue for you to explore.