
eBook - ePub
Pediatric Imaging for the Emergency Provider E-Book
Robert Vezzetti, Jestin Carlson, Debra Pennington
This is a test
Buch teilen
- 400 Seiten
- English
- ePUB (handyfreundlich)
- Über iOS und Android verfügbar
eBook - ePub
Pediatric Imaging for the Emergency Provider E-Book
Robert Vezzetti, Jestin Carlson, Debra Pennington
Angaben zum Buch
Buchvorschau
Inhaltsverzeichnis
Quellenangaben
Über dieses Buch
Children and infants comprise up to 20% of emergency department visits, and emergency physicians must be knowledgeable in choosing the most appropriate imaging modality to arrive at an accurate diagnosis and provide optimal patient care. Written specifically for the non-specialist and those with limited pediatric training, Pediatric Imaging for the Emergency Provider provides expert guidance in this challenging area. Abundant high-quality imaging examples cover the full range of pediatric disorders you're likely to see, including trauma, musculoskeletal, pulmonary, ENT, cardiac, genitourinary, gastroenterology, neurological, and neonatal patients.
- Presents more than 80 common and important rare cases, supported with 450+ images across relevant modalities including ultrasound, radiography, CT, and MRI.
- Identifies key radiographic findings for various pediatric conditions including congenital heart lesions, surgical entities, infectious disease processes, and traumatic injuries.
- Accompanies images with clear, concise text that makes it easy to grasp the most clinically significant points of each case.
- Provides expert guidance on best practices in important areas of pediatric imaging such as sedation, ionizing radiation exposure reduction, and imaging modality selection.
Häufig gestellte Fragen
Wie kann ich mein Abo kündigen?
Gehe einfach zum Kontobereich in den Einstellungen und klicke auf „Abo kündigen“ – ganz einfach. Nachdem du gekündigt hast, bleibt deine Mitgliedschaft für den verbleibenden Abozeitraum, den du bereits bezahlt hast, aktiv. Mehr Informationen hier.
(Wie) Kann ich Bücher herunterladen?
Derzeit stehen all unsere auf Mobilgeräte reagierenden ePub-Bücher zum Download über die App zur Verfügung. Die meisten unserer PDFs stehen ebenfalls zum Download bereit; wir arbeiten daran, auch die übrigen PDFs zum Download anzubieten, bei denen dies aktuell noch nicht möglich ist. Weitere Informationen hier.
Welcher Unterschied besteht bei den Preisen zwischen den Aboplänen?
Mit beiden Aboplänen erhältst du vollen Zugang zur Bibliothek und allen Funktionen von Perlego. Die einzigen Unterschiede bestehen im Preis und dem Abozeitraum: Mit dem Jahresabo sparst du auf 12 Monate gerechnet im Vergleich zum Monatsabo rund 30 %.
Was ist Perlego?
Wir sind ein Online-Abodienst für Lehrbücher, bei dem du für weniger als den Preis eines einzelnen Buches pro Monat Zugang zu einer ganzen Online-Bibliothek erhältst. Mit über 1 Million Büchern zu über 1.000 verschiedenen Themen haben wir bestimmt alles, was du brauchst! Weitere Informationen hier.
Unterstützt Perlego Text-zu-Sprache?
Achte auf das Symbol zum Vorlesen in deinem nächsten Buch, um zu sehen, ob du es dir auch anhören kannst. Bei diesem Tool wird dir Text laut vorgelesen, wobei der Text beim Vorlesen auch grafisch hervorgehoben wird. Du kannst das Vorlesen jederzeit anhalten, beschleunigen und verlangsamen. Weitere Informationen hier.
Ist Pediatric Imaging for the Emergency Provider E-Book als Online-PDF/ePub verfügbar?
Ja, du hast Zugang zu Pediatric Imaging for the Emergency Provider E-Book von Robert Vezzetti, Jestin Carlson, Debra Pennington im PDF- und/oder ePub-Format sowie zu anderen beliebten Büchern aus Medicina & Medicina de emergencia y cuidado crítico. Aus unserem Katalog stehen dir über 1 Million Bücher zur Verfügung.
Information
SECTION 1
Neonatal
Outline
- 4. My, what a big thymus you have! Neonate/infant mediastinal masses
- 5. A wheezin’ we will go: Bronchiolitis/viral pathology
- 6. Twisting the night away: Malrotation
- 7. Double bubble. . . double trouble! Duodenal obstruction
- 8. Cyanotic and acyanotic congenital heart disease
- 9. More than constipation: Failure to pass meconium
- 10. Rumbly in the tumbly: Pneumatosis intestinalis and necrotizing enterocolitis
4: My, what a big thymus you have! Neonate/infant mediastinal masses
Robert Vezzetti, MD, FAAP, FACEP
Case presentation
An 8-month-old male presents with 2 months of cough and intermittent rhinorrhea. He has been seen multiple times by his primary care provider and has been diagnosed at various times with viral upper respiratory tract infection and acute otitis media, for which he has been prescribed oral antibiotics. He has had some intermittent fevers as well, all of which have resolved after several days. There has been no travel or sick contacts, nor has there been any history of choking or concern for foreign body ingestion.
Physical examination reveals a thin but well-appearing and active child. He is afebrile and his vital signs are unremarkable, except for mild tachypnea (65 breaths per minute). There is no rhinorrhea and the oropharynx is clear. His chest demonstrates decreased breath sounds to the upper left chest, but there are no crackles, retractions, grunting, or stridor. He has a normal abdominal examination.
Imaging considerations
Plain radiography
This imaging modality is the most commonly utilized imaging modality for the neonatal or infant chest.1 Two views are preferred (anterior-posterior [AP] and lateral) when possible. Plain radiography may suggest the presence of a chest mass, prompting the use of advanced imaging. Ninety percent of chest masses can be visualized by plain radiography.2
Plain radiography is the first-line imaging modality when chest masses are suspected.3 However, this modality may miss small masses, and further imaging is indicated when a mediastinal mass is suspected, since a diagnosis is not usually made by plain radiography alone.3
Ultrasound (US)
This imaging modality is increasingly used for the evaluation of specific chest conditions. Examples include pneumothorax, pleural effusion, hemothorax, and chest masses.1 US of the mediastinum is limited, however, in patients above 5 years of age due to poor acoustic windows.3 The lack of exposure to ionizing radiation, rapidity, availability, and no need for sedation are all advantages of sonography.
Computed tomography (CT)
This imaging modality is typically utilized when plain radiography is abnormal and further delineation of a suspected chest mass is indicated. CT is also used for surgical planning when indicated.1 CT is readily available and rapid and usually does not require sedation. CT does include exposure to ionizing radiation, and appropriate pediatric imaging protocols should be utilized to reduce this exposure as much as possible.
CT is often utilized in patients with mediastinal masses. It has been shown to be very accurate for the characterization of masses (such as size and location) and to determine whether there is involvement of adjacent structures.2–4 CT can differentiate between cystic and solid structures and can evaluate for the presence of calcification, fat, or vascular components.2 CT findings have been shown to impact management in 65% of cases and have added additional diagnostic information in 82%.3,4
Magnetic resonance imaging (MRI)
As with CT, MRI is used for further anatomic definition and tissue characterization of suspected chest masses. MRI is particularly good at differentiating cystic from solid structures, especially compared to CT.2,3 MRI may also be used when planning surgical procedures.1 Availability and the need for sedation are potential disadvantages of MRI.
Positron emission tomography (PET)
PET is not a first-line imaging modality for diagnosing mediastinal masses in pediatric patients. However, PET imaging, including PET-CT or PET-MRI, can be used in staging tumors and monitoring response to therapy.3,5 Such imaging for children, though, is usually found at tertiary pediatric centers and generally is not widely available.
Imaging findings
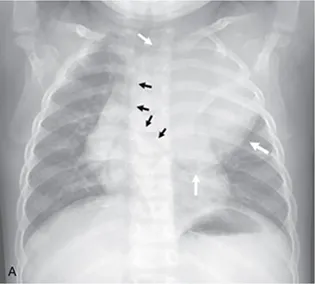
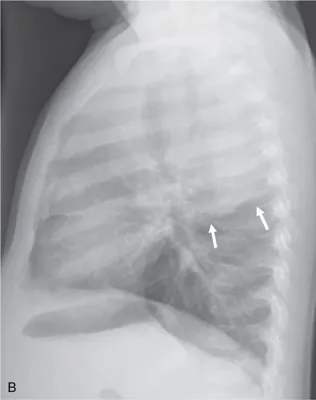
The patient had two-view plain radiography of the chest performed. There is a large rounded opacity in the left mid to upper chest that has a well-defined border laterally and inferiorly. There is mass effect on the lower trachea (displacement to the right) and left mainstem bronchus (displaced inferiorly and medially) (Fig. 4.1).
Case conclusion
The patient was admitted with consultation by Pediatric Oncology and Pediatric Surgery. A contrast-enhanced CT scan of the chest was obtained, demonstrating the mass, which appears centered in the posterior left mediastinum but extends to involve the middle and anterior mediastinum (Fig. 4.2). CT-guided biopsy revealed that ...