Surgical anatomy of the lateral transpsoas approach to the lumbar spine E-Book
eBook - ePub
Surgical anatomy of the lateral transpsoas approach to the lumbar spine E-Book
- 256 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Surgical anatomy of the lateral transpsoas approach to the lumbar spine E-Book
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
NeurosurgeryChapter 1
Superficial Nerves of the Anterolateral Abdominal Wall and the Lateral Transpsoas Approach to the Lumbar Spine
Mary Katherine Cleveland, Joe Iwanaga, and R. Shane Tubbs
Abstract
Lateral approaches to the lumbar spine have increased in popularity and offer an additional option to surgeons. However, these approaches demand a good working knowledge of regional anatomy in order to avoid complications. Herein, we describe the anatomy of the superficial nerves related to this approach.
Keywords
Anatomy; Lumbar; Spine; Surgery; Complications
Introduction
The lateral transpsoas approach to the lumbar spine is increasingly being used to treat degenerative changes requiring fusion (Arnold et al., 2012). In contrast to conventional posterior spinal fusion techniques, this minimally invasive approach spares extensive posterior tissue dissection and resection and decreases operative time, blood loss, postoperative pain, and tissue trauma. Although minimally invasive, this procedure has the approach-related risk to cause lumbar plexus nerve injuries secondary to the insertion and dilation of dilatators or retractors. Plexus injuries are reported in up to approximately 30% of patients, often presenting as neuropathic pain and motor or sensory deficits (Arnold et al., 2012; Pumberger et al., 2012; Rodgers et al., 2011).
Several anatomical studies on plexus nerve anatomy for lateral approaches have been published (Uribe et al., 2010; Benglis et al., 2009); however, few have systematically documented the types of injury typically observed at each spinal level after such procedures. In our earlier study, approximately 50% of all operated-upon segments had plexus nerve injuries occurring at segments L1–L4 and involving nerve roots as well as motor and sensory nerves (Grunert et al., 2017).
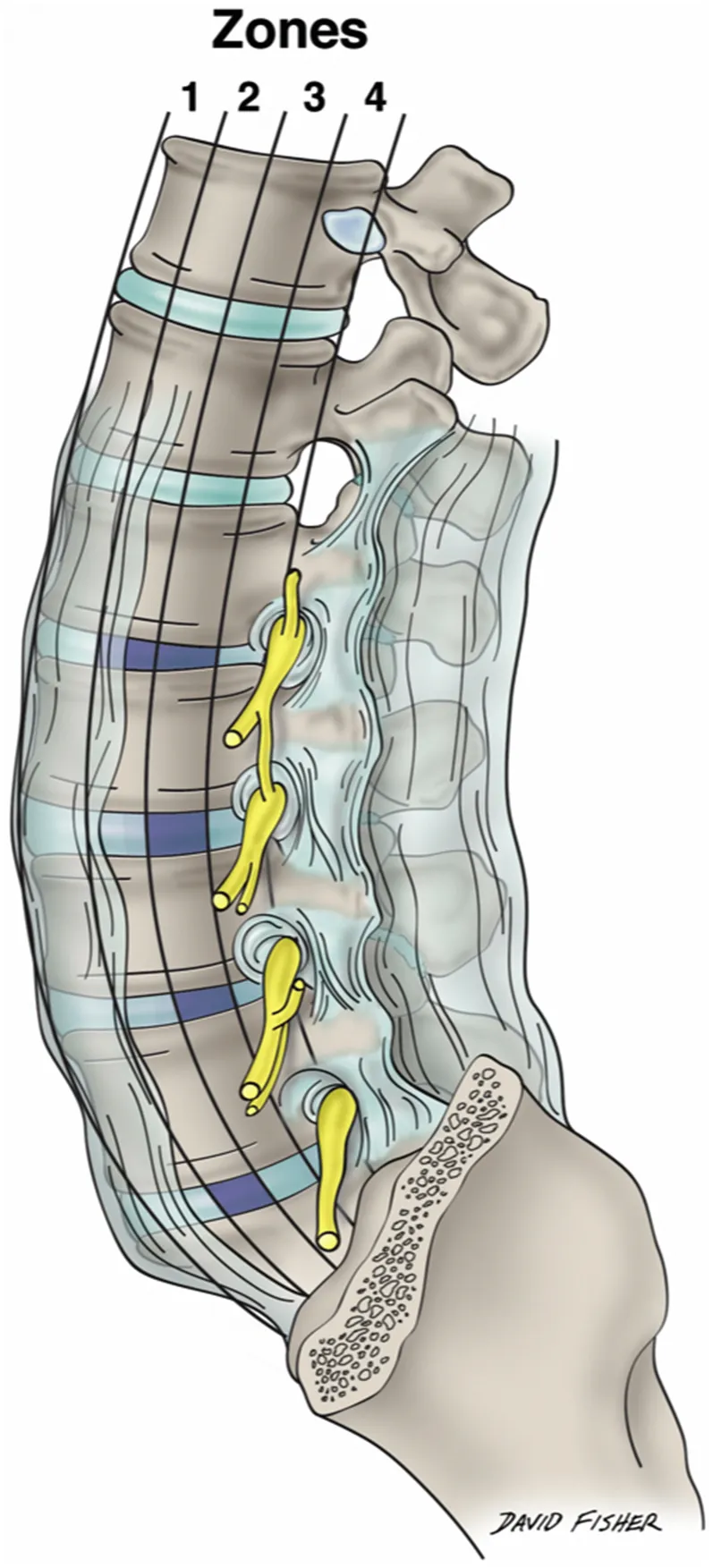
Moro and Uribe et al. subdivided each lumbar vertebral segment into four quarters (zone I to zone IV) from the anterior to the posterior border of the vertebral body (Fig. 1.1) (Uribe et al., 2010; Moro et al., 2003). Although describing the relationship of the plexus nerves to the lateral vertebral body surface helps in determining ideal docking points, it oversimplifies the complex plexus anatomy, as the nerves run in anteroposterior, superolateral, and mediolateral directions. As shown in the study of Grunert et al., injuries can occur throughout the entire trajectory of the lateral transpsoas approach to the lumbar spine. Over 50% of the nerve injuries occurred either at the lateral aspect of the psoas major muscle, within the outer abdominal muscles, or in the subcutaneous tissue of the abdominal wall, predominantly affecting the subcostal, ilioinguinal, iliohypogastric, and lateral femoral cutaneous nerves (Grunert et al., 2017).
As the superficial nerves of the region between the iliac crest and 12th rib are so concentrated (Fig. 1.2) and important to avoid with the lateral transpsoas approach to the lumbar spine, this chapter focuses on these structures and their detailed anatomy.
Segmental Lateral Cutaneous Branches
The skin and muscles of the anterolateral abdominal wall are innervated by the ventral rami of T7–T12. The muscles here also receive fibers from at least L1 ventral ramus and, as we have reported, as inferior as an L4 contribution. The lower thoracic and L1 nerves and their branches travel into the abdominal wall between the transversus abdominis and internal abdominal oblique muscles. Distally, they pierce the rectus sheath. Along their course, the nerves supply not only the skin and adjacent musculature but also the parietal peritoneum. These nerves give rise to lateral and anterior cutaneous branches (Figs. 1.3 and 1.4). The former arise at about the anterior axillary line and pierce the anterolateral muscles of the abdominal wall near the midaxillary line. As the lateral cutaneous branches of these nerves reach the skin, they split into anterior and posterior branches. The anterior cutaneous branches are the terminal branches of each of these segmental nerves and exit the rectus sheath anteriorly to reach the overlying skin where they too split into branches, medial and lateral.
Superior Cluneal Nerves
The superior cluneal nerves (SCNs) (Figs. 1.5–1.8) are the posterior cutaneous branches (from the lateral branch) of the dorsal rami usually described as arising from the upper three lumbar spinal nerves. Historically, it has been believed that the origin of the SCN is the dorsal rami of the L1, L2, and L3 spinal nerves. The SCN is usually depicted as having three branches: medial, intermediate, and lateral SCN.
Out of 20 sides, we previously reported the vertebral level of the origin of the SCN was T12 on 2 sides (10%), L1 on 15 sides (75%), L2 on 18 sides (90%), L3 on 19 sides (95%), L4 on 9 sides (45%) (Fig. 1.9), and L5 on 2 sides (10%), respec...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- List of Contributors
- Preface
- Chapter 1. Superficial Nerves of the Anterolateral Abdominal Wall and the Lateral Transpsoas Approach to the Lumbar Spine
- Chapter 2. Muscles of the Anterolateral Abdominal Wall
- Chapter 3. The Posterior Abdominal Wall and Retroperitoneum
- Chapter 4. Posterior Abdominal Wall Muscles
- Chapter 5. The Diaphragm
- Chapter 6. Lumbar Plexus
- Chapter 7. Lumbar Vertebrae
- Chapter 8. Lumbar Intervertebral Discs
- Chapter 9. The Ligaments of the Lumbar Spine
- Chapter 10. The Lumbar Intervertebral Foramina
- Chapter 11. Sectional Anatomy for the Lateral Transpsoas Approach to the Lumbar Spine: A Pictorial Guide
- Chapter 12. The Sympathetic Trunk in the Abdomen
- Chapter 13. The Lumbosacral Trunk and Tunnel
- Chapter 14. Lateral Transpsoas Approaches to the Lumbar Spine and the Kidney, Ureter, and Colon
- Chapter 15. Lymphatics of the Abdomen
- Chapter 16. Anatomical Variations Relevant to the Lateral Transpsoas Approach to the Lumbar Spine
- Chapter 17. Technique: Lateral Transpsoas Approaches to the Lumbar Spine
- Chapter 18. Autonomics of the Abdomen
- Chapter 19. The Abdominal Aorta
- Chapter 20. The Inferior Vena Cava and Its Branches and Connections in the Abdomen
- Chapter 21. Lateral Approaches to the Thoracolumbar Junction—Anatomical Considerations
- Chapter 22. Lateral Approaches to the Thoracic Spine
- Chapter 23. Techniques for the Lateral Thoracolumbar Approach
- Chapter 24. Complications From Lateral Transpsoas Approaches to the Lumbar Spine
- Chapter 25. Tips and Tricks of Lateral Approaches to the Thoracolumbar Spine
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Surgical anatomy of the lateral transpsoas approach to the lumbar spine E-Book by R. Shane Tubbs,Rod J. Oskouian Jr.,Joe Iwanaga,Marc Moisi,Rod J. Oskouian, Jr., R. Shane Tubbs, Rod J. Oskouian, Jr., Joe Iwanaga, Marc Moisi in PDF and/or ePUB format, as well as other popular books in Medicine & Neurosurgery. We have over 1.5 million books available in our catalogue for you to explore.