
eBook - ePub
Surgical anatomy of the lateral transpsoas approach to the lumbar spine E-Book
R. Shane Tubbs, Rod J. Oskouian, Jr., Joe Iwanaga, Marc Moisi
This is a test
Partager le livre
- 256 pages
- English
- ePUB (adapté aux mobiles)
- Disponible sur iOS et Android
eBook - ePub
Surgical anatomy of the lateral transpsoas approach to the lumbar spine E-Book
R. Shane Tubbs, Rod J. Oskouian, Jr., Joe Iwanaga, Marc Moisi
Détails du livre
Aperçu du livre
Table des matières
Citations
À propos de ce livre
Surgical anatomy of the lateral transpsoas approach to the lumbar spine E-Book
Foire aux questions
Comment puis-je résilier mon abonnement ?
Il vous suffit de vous rendre dans la section compte dans paramètres et de cliquer sur « Résilier l’abonnement ». C’est aussi simple que cela ! Une fois que vous aurez résilié votre abonnement, il restera actif pour le reste de la période pour laquelle vous avez payé. Découvrez-en plus ici.
Puis-je / comment puis-je télécharger des livres ?
Pour le moment, tous nos livres en format ePub adaptés aux mobiles peuvent être téléchargés via l’application. La plupart de nos PDF sont également disponibles en téléchargement et les autres seront téléchargeables très prochainement. Découvrez-en plus ici.
Quelle est la différence entre les formules tarifaires ?
Les deux abonnements vous donnent un accès complet à la bibliothèque et à toutes les fonctionnalités de Perlego. Les seules différences sont les tarifs ainsi que la période d’abonnement : avec l’abonnement annuel, vous économiserez environ 30 % par rapport à 12 mois d’abonnement mensuel.
Qu’est-ce que Perlego ?
Nous sommes un service d’abonnement à des ouvrages universitaires en ligne, où vous pouvez accéder à toute une bibliothèque pour un prix inférieur à celui d’un seul livre par mois. Avec plus d’un million de livres sur plus de 1 000 sujets, nous avons ce qu’il vous faut ! Découvrez-en plus ici.
Prenez-vous en charge la synthèse vocale ?
Recherchez le symbole Écouter sur votre prochain livre pour voir si vous pouvez l’écouter. L’outil Écouter lit le texte à haute voix pour vous, en surlignant le passage qui est en cours de lecture. Vous pouvez le mettre sur pause, l’accélérer ou le ralentir. Découvrez-en plus ici.
Est-ce que Surgical anatomy of the lateral transpsoas approach to the lumbar spine E-Book est un PDF/ePUB en ligne ?
Oui, vous pouvez accéder à Surgical anatomy of the lateral transpsoas approach to the lumbar spine E-Book par R. Shane Tubbs, Rod J. Oskouian, Jr., Joe Iwanaga, Marc Moisi en format PDF et/ou ePUB ainsi qu’à d’autres livres populaires dans Medicine et Neurosurgery. Nous disposons de plus d’un million d’ouvrages à découvrir dans notre catalogue.
Informations
Sujet
MedicineSous-sujet
NeurosurgeryChapter 1
Superficial Nerves of the Anterolateral Abdominal Wall and the Lateral Transpsoas Approach to the Lumbar Spine
Mary Katherine Cleveland, Joe Iwanaga, and R. Shane Tubbs
Abstract
Lateral approaches to the lumbar spine have increased in popularity and offer an additional option to surgeons. However, these approaches demand a good working knowledge of regional anatomy in order to avoid complications. Herein, we describe the anatomy of the superficial nerves related to this approach.
Keywords
Anatomy; Lumbar; Spine; Surgery; Complications
Introduction
The lateral transpsoas approach to the lumbar spine is increasingly being used to treat degenerative changes requiring fusion (Arnold et al., 2012). In contrast to conventional posterior spinal fusion techniques, this minimally invasive approach spares extensive posterior tissue dissection and resection and decreases operative time, blood loss, postoperative pain, and tissue trauma. Although minimally invasive, this procedure has the approach-related risk to cause lumbar plexus nerve injuries secondary to the insertion and dilation of dilatators or retractors. Plexus injuries are reported in up to approximately 30% of patients, often presenting as neuropathic pain and motor or sensory deficits (Arnold et al., 2012; Pumberger et al., 2012; Rodgers et al., 2011).
Several anatomical studies on plexus nerve anatomy for lateral approaches have been published (Uribe et al., 2010; Benglis et al., 2009); however, few have systematically documented the types of injury typically observed at each spinal level after such procedures. In our earlier study, approximately 50% of all operated-upon segments had plexus nerve injuries occurring at segments L1–L4 and involving nerve roots as well as motor and sensory nerves (Grunert et al., 2017).
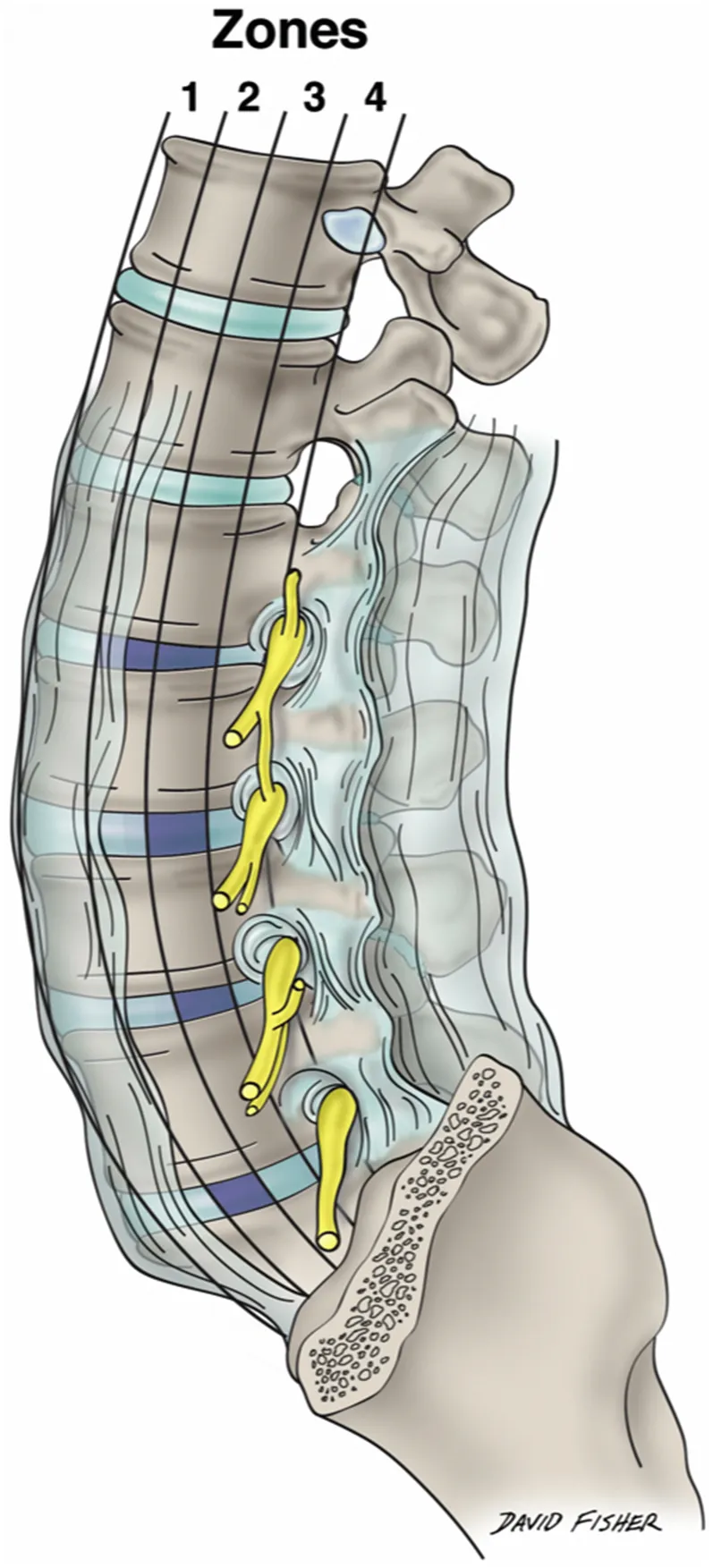
Moro and Uribe et al. subdivided each lumbar vertebral segment into four quarters (zone I to zone IV) from the anterior to the posterior border of the vertebral body (Fig. 1.1) (Uribe et al., 2010; Moro et al., 2003). Although describing the relationship of the plexus nerves to the lateral vertebral body surface helps in determining ideal docking points, it oversimplifies the complex plexus anatomy, as the nerves run in anteroposterior, superolateral, and mediolateral directions. As shown in the study of Grunert et al., injuries can occur throughout the entire trajectory of the lateral transpsoas approach to the lumbar spine. Over 50% of the nerve injuries occurred either at the lateral aspect of the psoas major muscle, within the outer abdominal muscles, or in the subcutaneous tissue of the abdominal wall, predominantly affecting the subcostal, ilioinguinal, iliohypogastric, and lateral femoral cutaneous nerves (Grunert et al., 2017).
As the superficial nerves of the region between the iliac crest and 12th rib are so concentrated (Fig. 1.2) and important to avoid with the lateral transpsoas approach to the lumbar spine, this chapter focuses on these structures and their detailed anatomy.
Segmental Lateral Cutaneous Branches
The skin and muscles of the anterolateral abdominal wall are innervated by the ventral rami of T7–T12. The muscles here also receive fibers from at least L1 ventral ramus and, as we have reported, as inferior as an L4 contribution. The lower thoracic and L1 nerves and their branches travel into the abdominal wall between the transversus abdominis and internal abdominal oblique muscles. Distally, they pierce the rectus sheath. Along their course, the nerves supply not only the skin and adjacent musculature but also the parietal peritoneum. These nerves give rise to lateral and anterior cutaneous branches (Figs. 1.3 and 1.4). The former arise at about the anterior axillary line and pierce the anterolateral muscles of the abdominal wall near the midaxillary line. As the lateral cutaneous branches of these nerves reach the skin, they split into anterior and posterior branches. The anterior cutaneous branches are the terminal branches of each of these segmental nerves and exit the rectus sheath anteriorly to reach the overlying skin where they too split into branches, medial and lateral.
Superior Cluneal Nerves
The superior cluneal nerves (SCNs) (Figs. 1.5–1.8) are the posterior cutaneous branches (from the lateral branch) of the dorsal rami usually described as arising from the upper three lumbar spinal nerves. Historically, it has been believed that the origin of the SCN is the dorsal rami of the L1, L2, and L3 spinal nerves. The SCN is usually depicted as having three branches: medial, intermediate, and lateral SCN.
Out of 20 sides, we previously reported the vertebral level of the origin of the SCN was T12 on 2 sides (10%), L1 on 15 sides (75%), L2 on 18 sides (90%), L3 on 19 sides (95%), L4 on 9 sides (45%) (Fig. 1.9), and L5 on 2 sides (10%), respec...