The book includes 100 cases (common and rare) with highly organised radiological description of the diseases.
The cases are grouped into three chapters: Upper Limbs, Neck/Trunk/Spine and Lower Limbs.
High quality images (X-ray, US, CT and MRI).
It covers all imaging modalities including conventional radiology, ultrasound/Doppler, CT scan and MRI.
The topics covered in the book represent the common and important diseases encountered in musculoskeletal imaging.
The material presented for each case provides a thorough and comprehensive description of the disease entity, enabling the radiologist or the clinician to develop a clear concept of the entity through the different imaging modalities that are present.
What is interesting in this book is one case per page. The book can be used as a mean of rapid revision of a large number of cases in a short time or as a test of knowledge by masking the radiological description and diagnosis and trying by using the clinical data and radiological images to describe first the pathology then propose a diagnosis.
- 244 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineCase 1
Clinical Presentation
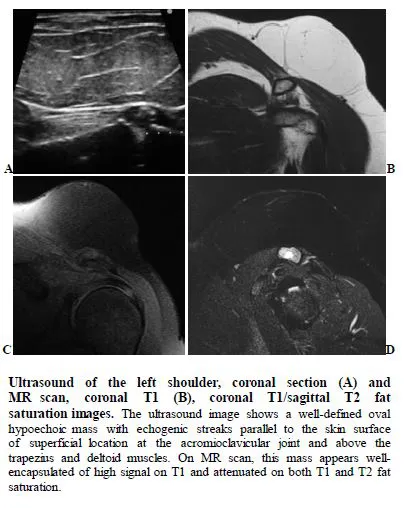
A 29-year-old male patient with no past medical history had observed a rapidly growing mass of his left shoulder and slight soreness during a period of four weeks after having performed physical exercise for several weeks in a fitness studio. The mass was palpable but deeply located in the ventral shoulder.
Radiological Findings
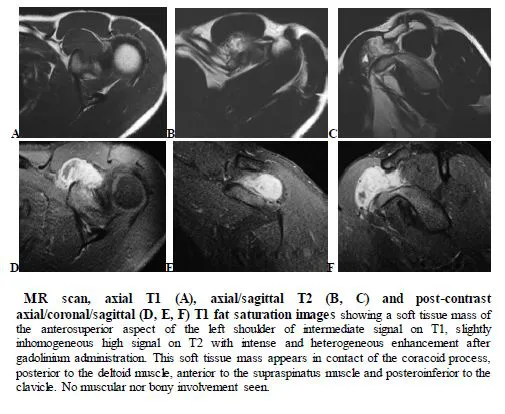
Diagnosis: Desmoid tumor
Desmoid tumors are benign lesions belonging to the group of fibromatoses. They arise from the connective tissue, fascia or muscular aponeurosis.
The etiology has not been sufficiently explained. Trauma, endocrine and genetic factors have been suggested to be predisposing factors. Although the tumors are benign, they show aggressive locoregional extension with destruction of surrounding structures leading to an increased morbidity. Tumors are mostly found in abdomen and by far are the commonest neoplasm of the abdominal wall. Only 7–15% occur in the head and neck areas.
Successful treatment can be achieved by surgical excision, radiation and with pharmacological agents. As this tumor is rare, recommendations for the optimal treatment algorithm is lacking.
Diagnosis can be made by US, CT, and MRI. Before planning any type of surgery, the extension of the tumor and its relation to neighboring neuro-vascular as well as functional structures need to be identified.
The lesions typically appear as hypoechoic homogeneous mass on ultrasound. They may appear isoechoic to muscle, may be lobulated, and may show signs of vascularity on color Doppler interrogation.
Most desmoid tumors are well-circumscribed lesions in CT, although in some cases they may appear more aggressive with ill-defined margins. Most lesions are relatively isodense and homogeneous or focally hyperattenuating compared to soft tissue on the non-contrast scan with enhancement following intravenous contrast.
On MRI, typically, the lesions appear of low signal intensity on T1 and T2 with homogeneous, non- homogeneous, or no significant enhancement following intravenous contrast. MRI is more sensitive to local tumor extension. Their appearance is accounted for their dense cellularity.
Case 2
Clinical Presentation
A 22-year-old male patient with history of repeated left shoulder dislocation, presented with shoulder pain and instability.
Radiological Findings
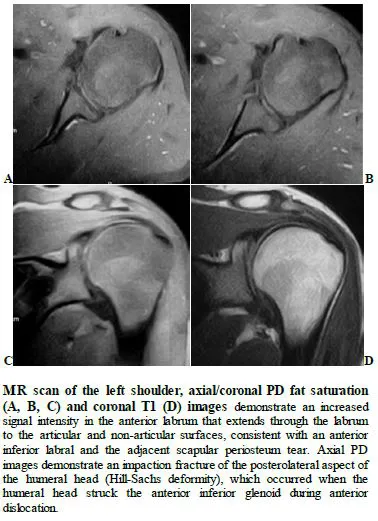
Diagnosis: Bankart lesion (bony Bankart)
The Bankart lesion is named after the English orthopedic surgeon, Arthur Blundell Bankart. The lesion is a common complication of anterior shoulder dislocation and frequently associated with a Hill-Sachs lesion.
Those result from detachment of the anteroinferior labrum from the underlying glenoid as a result of the anteriorly dislocated humeral head compressing against the labrum. It may only be isolated labral injury “Soft Bankart,” or involve the bony glenoid margin “Bony Bankart.” Soft Bankarts are more common than bony lesions.
The same mechanism of compression results in a Hill-Sachs lesion. Bankart and Hill-Sachs lesions often occur together than to be isolated. Bankart lesions do heal, and early surgical intervention may not be required. The labral fragment needs to be sutured back to the glenoid rim using suture anchors.
Bankart Variants:
- Perthes lesion of the shoulder: tear of the glenoid labrum with intact scapular periosteum
- Anterior labroligamentous periosteal sleeve avulsion (ALPSA): mobilized labrum remains attached to the glenoid periosteum.
Only bony Bankart lesion may be seen on plain radiograph as a fracture of the anteroinferior aspect of the glenoid.
Non-contrast CT may show fracture at the anteroinferior glenoid “Bony Bankart”. However, CT arthrography may be needed to visualize “Soft Bankart.”
A linear T2/PD high signal intensity coursing through the normal low signal anteroinferior labrum can be seen in MRI. A number of lesions may have similar appearances. “Double Axillary Pouch” sign on coronal MR arthrogram is a specific sign for an anteroinferior labral tear. MR may show displaced anterior glenoid labrum with bone, small or absent anterior labrum.
Case 3
Clinical Presentation
A 34-year-old female patient complaining of non-specific posterior pain and weakness of the left shoulder.
Radiological Findings
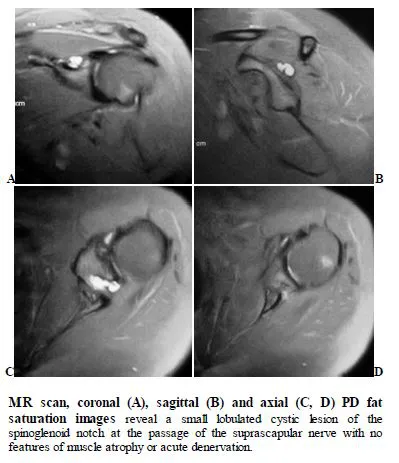
Diagnosis: Suprascapular neuropathy (or suprascapular nerve entrapment)
Suprascapular neuropathy results from compression or traction of the suprascapular nerve, typically at the suprascapular or spinoglenoid notch. Certain sports like weight lifting predisposes to this type of neuropathy. This may also be produced by mass effect from a ganglion cyst or any other neoplastic growth. The entrapment leads to supra and infraspinatus weakness and pain may be clinically difficult to differentiate from rotator cuff tear.
The nerve at suprascapular notch contains both motor and sensory branches. Proximal entrapment cause denervation changes involving both muscles whereas distal entrapment along the course of the nerve only involves the infraspinatus. Familiarity with the neurovascular anatomy is essential in analyzing the nerve entrapment.
Electromyography and nerve conduction velocity studies remain the gold standard for confirmation of suprascapular neuropathy. However, negative findings do not exclude it. Initial management is usually nonoperative, consisting of activity modification, physiotherapy, and nonsteroidal anti-inflammatory drugs. Surgical intervention is considered for patients with nerve compression by an external source or for symptoms refractory to conservative measures. Decompression of the suprascapular nerve may be accomplished through an open approach, although arthroscopic surgical approaches have become more common in recent years.
As the clinical presentation is confusing, the patient may be sent for MRI to rule out rotator cuff tear or other more common shoulder abnormalities. MRI is also an indispensable tool for evaluation of peripheral nerve injuries at the shoulder and muscle denervation changes. MRI is capable of showing the lesions at supraclavicular or spinoglenoid notch directly.
Muscle denervation can have several MRI appearances. In subacute phase, the affected muscle demonstrates increased T2-signal resulting from muscle edema. In the chronic stages, fatty infiltration usually accompanied by muscle atrophy representing irreversible muscle injury.
Case 4
Clinical Presentation
A 54-year-old female patient presented with a left shoulder mass, known since last 10 years and progressively increasing in size.
Radiological Findings
Diagnosis: Lipoma of left shoulder
Lipomas are well-capsulated benign soft tissue tumors representing almost 50% of all soft tissue tumors. They can be classified on the basis of their anatomical location, clinical evaluation or histological findings. Subcutaneous lipomas are the commonest. The intermuscular variants are also seen.
Superficial lipomas can be accurately diagnosed on the basis of clinical findings in up to 85% of cases. Those superficial lipomas are typically mobile, palpable, doughy, and solitary soft tissue mass. In 80% of cases, the superficial lipomas are smaller than 5 cm and only 1% is greater than 10 cm in size. They enlarge slowly and are frequently asymptomatic. Clinical symptoms are uncommon but they may cause local pain and tenderness, limitation of joint movement, and nerve compression.
It is unclear if a soft tissue lipoma represents a benign neoplasm or a local hyperplasia of fatty tissue or a combination of both. In 5–15% of patients, lipomas may be multiple. Multiple lipomas tend to be commoner in males. Lipomas commonly affect the upper back, neck, proximal extremities (particularly the shoulder), and abdomen. Lipomas around the shoulder are known to infiltrate between the muscles of the extremities and the thoracic wall. Surgical excision is still the best form of treatment if the lesion is symptomatic.
Small lipomas often may not be noticeable on radiography, while larger lipomas may show a typical radiolucency. Underlying osseous abnormalities are rare.
On US, lipomas appear as homogeneous hyperechoic lesion having no posterior acoustic enhancement.
Heterogeneity may be caused by septa or other non-lipomatous components.
CT appearance of a superficial lipoma is a circumscribed low-density lesion. Areas of calcification raise the suspicion of well-differenti...
Table of contents
- Musculoskeletal Imaging
- About the Authors
- Dedication
- Copyright Information ©
- Acknowledgements
- Contributors
- Foreword
- Preface
- Upper Limbs
- Case 1
- Case 2
- Case 3
- Case 4
- Case 5
- Case 6
- Case 7
- Case 8
- Case 9
- Case 10
- Case 11
- Case 12
- Case 13
- Case 14
- Case 15
- Case 16
- Case 17
- Case 18
- Case 19
- Case 20
- Case 21
- Case 22
- Case 23
- Case 24
- Case 25
- Case 26
- Case 27
- Case 28
- Spine and Trunk
- Case 29
- Case 30
- Case 31
- Case 32
- Case 33
- Case 34
- Case 35
- Case 36
- Case 37
- Case 38
- Case 39
- Case 40
- Case 41
- Case 42
- Case 43
- Case 44
- Lower Limbs
- Case 45
- Case 46
- Case 47
- Case 48
- Case 49
- Case 50
- Case 51
- Case 52
- Case 53
- Case 54
- Case 55
- Case 56
- Case 57
- Case 58
- Case 59
- Case 60
- Case 61
- Case 62
- Case 63
- Case 64
- Case 65
- Case 66
- Case 67
- Case 68
- Case 69
- Case 70
- Case 71
- Case 72
- Case 73
- Case 74
- Case 75
- Case 76
- Case 77
- Case 78
- Case 79
- Case 80
- Case 81
- Case 82
- Case 83
- Case 84
- Case 85
- Case 86
- Case 87
- Case 88
- Case 89
- Case 90
- Case 91
- Case 92
- Case 93
- Case 94
- Case 95
- Case 96
- Case 97
- Case 98
- Case 99
- Case 100
- References
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Musculoskeletal Imaging by Ammar Haouimi in PDF and/or ePUB format, as well as other popular books in Medicine & Radiology, Radiotherapy & Nuclear Medicine. We have over 1.5 million books available in our catalogue for you to explore.