Social work law is at the foundation of all social work practice, from shaping professional boundaries to determining the level of intervention. Every case is complex and unique and therefore requires different legal treatment; this means it is absolutely vital that social workers not only understand the law, but are able to critically analyse the legal framework and apply it to their practice.
This book provides students and practitioners with an essential guide to adult social care law. It lays out the key case law, core legislation and the HSPCC standards as they apply to different areas of adult social care. This includes issues of capacity, making an assessment, supporting carers and working with vulnerable adults. Designed to support learning needs, the book is packed with engaging case studies and reflective exercises, as well as a legal toolbox to help simplify the legal jargon.
Whether you are a student or practitioner, this is a practical, accessible guide to competent and lawful practice in adult social care.
- 216 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Adult Social Care Law in England
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
chapter 1
Social Work Practice and the Law
In this chapter, you will learn about:
■ The organizational and administrative framework
■ Community care services
■ Directions and guidance
■ Powers and duties
■ Human Rights Act 1998
■ Anti-discrimination
■ Director of Social Services
■ Social work practice and the law
■ Delegated and designated functions
■ Registration of social workers
■ Standards of proficiency
■ Partnership and coordination
■ Accountability
■ Conclusion
Remember to consult The Legal Toolbox on pp. xiii–xx. This will help you to understand processes and procedures referred to in this chapter.
Introduction
Social work law is the basis of social work practice. It determines the organizational setting in which social work takes place; it defines what social workers are employed to do; and, by setting out what redress is available when things go wrong, it determines the boundaries of social work action and the nature and extent of social work accountability. It is the law that defines the individuals towards whom social workers have responsibilities, such as, vulnerable adults and their carers, and which determines, often in broad terms, the nature and extent of social work intervention (such as prevention, protection and rehabilitation). The law also sets out the conditions under which compulsory intervention is permissible, as well as the safeguards that should ensure that such intervention takes place in accordance with due process and in adherence to human rights. An important aspect of the social work task is to determine appropriate levels of support, care, protection and control, taking into account the inevitable constraints imposed by the availability of resources. It is the law, too, that identifies the strategic aims and objectives that underpin the delivery of services, both nationally and locally. In essence, social work law consists of three elements: a set of organizational and administrative processes and procedures; a specific body of statutes and judicial decisions; and a body of professional ethics and values. The law provides ‘the essential bone structure of social work practice’ (Roberts and Preston-Shoot 2000) and so helps to determine its nature and character.
Table 1.1 Number of clients receiving community-based services by type
18–64 | 65 and over | |
Day care | 77,000 | 83,000 |
Direct payments | 78,000 | 61,000 |
Equipment and adaptations | 100,000 | 330,000 |
Home care | 103,000 | 415,000 |
Meals | 4,000 | 56,000 |
Other | 5,000 | 62,000 |
Professional support | 166,000 | 102,000 |
Short-term residential (not respite) | 13,000 | 57,000 |
Source: Health and Social Care Information Centre (2013a).
Table 1.2 Number of people in residential and nursing care by type of accommodation
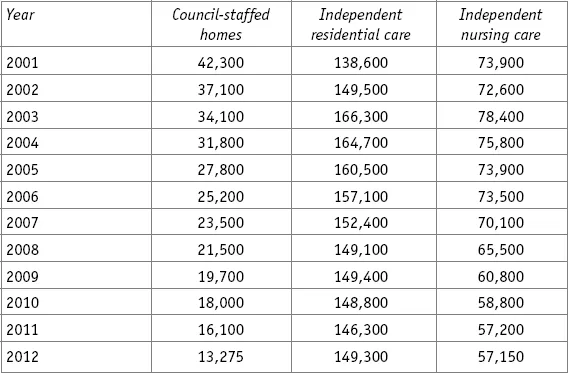
Source: Health and Social Care Information Centre (2013a).
Significant numbers of people rely on social services, either partially or completely. For example, Tables 1.1 and 1.2 present the number of people receiving domiciliary and residential/nursing care.
Given these numbers, it is crucial that social workers understand the nature and extent of their legal mandate, and how it affects the lives of those who need their help or support.
The organizational and administrative framework
The administrative and organizational framework for the delivery of social services is to be found mainly in the Local Authority Social Services Act 2000 (LASSA 1970), as amended, and the Local Government Act 2000 (LGA 2000).
The law recognizes the concept of an artificial legal person created by an Act of Parliament. Legal persons of this kind are collectively known as ‘corporations’, of which local authorities are an important example. As such, local authorities are capable of assuming legal powers and responsibilities to enable them to provide or arrange a range of services in their locality. The structure of local government in England is complex and varied. However, s.1 LASSA 1970, identifies the units of local government with legal responsibility for providing or arranging social services in their area. These consist currently of the metropolitan districts (such as Sheffield and Wolverhampton) and the London boroughs (such as Wandsworth and Brent, and the City of London Council); the county councils (such as, Lancashire and Kent); and the unitary authorities (such as Cornwall and Shropshire) (s.1 LASSA 1970, as amended). For ease of reference, these will be referred to as Councils with Social Services Responsibilities (CSSR). The LGA 2000 requires such authorities to set up an executive structure with decision-making powers and responsibilities, including the provision of social services that are required to undertaken under s.1A LASSA 1970. The Secretary of State may designate other social services functions to be performed by these local authorities.
A significant feature of the development of social services over the past few years has been the increased involvement of the independent sector in the provision of services; that is, profit-making organizations, as well as voluntary organizations. The Griffiths Report and the subsequent National Health Service and Community Care Act 1990 (NHSCCA 1990) developed a more open market for the provision of community care and residential care for adults (Griffiths 1988). Table 1.2 shows that residential care provided directly by local authorities represents a small proportion of the total provision. As Figure 1.1 shows, for domiciliary care the major provider is the independent sector.
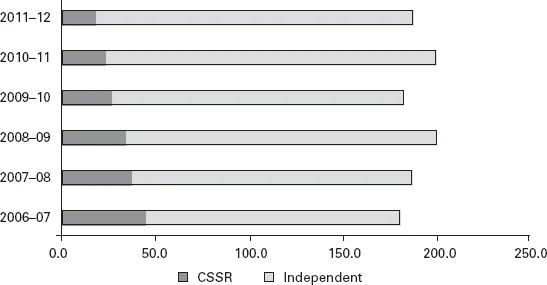
Figure 1.1 Contact hours in millions for home care provided during the year, by sector, 2006–07 to 2011–12
Source: Health and Social Care Information Centre (2013a).
Exercise 1.1
Choose a local authority with social services responsibility and identify the following characteristics:
■ The demography of the local authority area (structure of population: age, disability, gender, ethnicity, etc.) and its economic profile (e.g. unemployment levels, social housing, and indicators of deprivation).
■ The level of expenditure on social services for the area and how it is distributed between various groups (e.g. children, older people, mental health, learning disability).
Much of this data should be available on the authority’s website.
1. Do you consider this information is easily accessible to members of the public?
2. Are there any gaps in the information provided by the authority?
Community care services
As defined in s.46(3) NHSCCA 1990, ‘community care services’ for adults are services that a local authority may provide or arrange to be provided in its area under:
■ ss.21–29, Part III, National Assistance Act 1948.
■ s.45 Health Services and Public Health Act 1968.
■ s.254 and Schedule 20 National Health Service Act 2006.
■ s.117 Mental Health Act 1983.
Since the NHSCCA 1990, further legislation has come into force (such as the Equality Act 2010 (EA 2010) plus no fewer than three separate enactments relating to carers). These are discussed in the chapters that follow.
Directions and guidance
Much of the legislation concerning services for adults is set out in very general terms. More detailed provisions have been issued by the Department of Health in the form of Directions and Regulations and, exceptionally, in the form of Circulars. As long as they are properly made and issued, such documents often have, in practice, the same legal effect as the original legislation. They are open to challenge only if their contents are inconsistent with the terms of the original legislation, or the Human Rights Act 1998 (HRA 1998).
Another means by which gaps in the legislation are filled is through guidance issued by the Department of Health. Section 7 LASSA 1970, states that:
| “ | Local authorities shall, in the exercise of their social services functions, including the exercise of any discretion conferred by any relevant enactment, act under the general guidance of the Secretary of State. |
As will become apparent later in the book, a substantial amount of s.7 guidance has been issued. What is its legal significance? (See Box 1.1.)
The consequence of not following s.7 guidance is...
Table of contents
- Cover
- Title
- Copyright
- Contents
- List of Tables and Figures
- List of Case Examples and Boxes
- List of Abbreviations
- The Legal Toolbox
- Preface
- 1 Social Work Practice and the Law
- 2 Legal Capacity
- 3 Referral and Assessment
- 4 Community Care Services
- 5 Carers
- 6 Mental Health Law
- 7 Adult Safeguarding and Protection
- 8 Seeking Redress
- Appendix 1: Cases
- Appendix 2: Statutes and Statutory Instruments
- Bibliography
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Adult Social Care Law in England by John Williams,Gwyneth Roberts,Aled Griffiths in PDF and/or ePUB format, as well as other popular books in Politics & International Relations & Social Policy. We have over 1.5 million books available in our catalogue for you to explore.