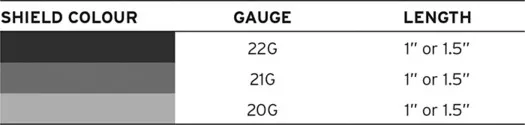
BD Vacutainer® needles are available with a 20, 21 or 22 gauge needle.
The higher the gauge, the narrower the diameter of the needle.
Colours are universal and can be applied to other vacutainer systems used in practice.
Patients requiring IV fluids should have a fluid or hydration assessment by senior medical or nursing staff at least once per 24 hours. Along with a physical examination, NICE (2013) recommends that their urea and electrolytes are checked daily.
Fluid status can be broadly categorised as euvolaemic (normal fluid status), hypovolaemic (dehydrated) and hypervolaemic (overloaded).
Euvolaemia: Patients with normal fluid status who are well hydrated and have no abnormal fluid losses.
Hypovolaemia: Also known as dehydration, hypovolaemic patients have too little circulating blood volume. The two broad causes of hypovolaemia are:
- output too high: losing too much fluid, e.g. diarrhoea
- input too low: inadequate fluid intake, e.g. swallowing difficulties.
Hypervolaemia: Commonly known as ‘overload’, patients experiencing hypervolaemia have too much fluid in their circulating volume. The two broad causes of hypervolaemia are:
- output too low: unable to make enough urine, e.g. chronic kidney disease
- input too high for body’s ability to handle the fluid, e.g. advanced heart failure.
Indications for IV fluids
Drinking is usually the preferred route for fluid intake; however, sometimes fluids require to be administered intravenously. The three main reasons for IV fluid administration are:
- routine maintenance
- replacement of fluid loss
- resuscitation.
Routine maintenance is for patients who are unable to meet their intake requirements orally. Adults require a routine fluid intake of 25–30 ml/kg/24 hours. Older or frail adults require less at 20–25 ml/kg/24 hours (NICE, 2013). Patients with hepatic, renal or cardiac impairment will have different requirements and should have their intake goals set and reviewed by senior medical staff.
Patients who are nil by mouth should be considered for routine maintenance if they are expected to be nil by mouth for longer than 8 hours.
Replacement fluids are given in addition to maintenance fluids to patients who have experienced either recent or ongoing fluid loss, e.g. high output stoma, vomiting and diarrhoea.
Resuscitation fluids are given in emergencies when rapid fluid administration is required to preserve the patient’s circulatory system, e.g. major haemorrhage.
Fluid Types
There are two types of IV fluids: crystalloids and colloids. Crystalloids consist of small molecules, which means that the fluid can leak out of the blood vessels into the surrounding tissues. Colloids have larger molecules that cannot leave the blood vessels so easily, which theoretically means that a smaller volume of infusion is required compared to crystalloid.
There is a move away from sodium chloride 0.9% towards increased use of balanced crystalloids, e.g. Hartmann’s solution. The contents of balanced crystalloids more closely resemble blood plasma than crystalloids such as sodium chloride 0.9% or glucose 5%.
Traditionally known as fluid balance charts, the main purpose of these charts is the assessment of intake and output rather than just overall fluid balance. For example, a patient who has an intake of 400 ml and output of 400 ml in 24 hours has both an inadequate fluid intake and output but would have a neutral fluid balance.
Totalling should take advantage of existing work patterns, e.g. before the ward doctor’s handover to the out-of-hours team, or before the day shift handover to the night shift, to help ensure prompt identification and resolution of issues.