What Is Vaginismus/GPPPD?
According to the DSM-IV (American Psychiatric Association, 2000), which is the diagnostic manual that psychologists and other mental health professionals follow in their assessment and diagnosis of psychological disorders, vaginismus is defined as:
In other words, vaginismus is a condition where the woman consistently experiences involuntary contractions of her vaginal muscles which causes difficulties with penetration and leads to significant personal or relationship distress.
Often vaginismus makes penis-in-vagina (PIV) sex impossible and can be the cause of an unconsummated marriage. Although the muscular spasms that occur in vaginismus can help the condition be diagnosed (by a qualified gynecologist, pelvic physical therapist, or family doctor), diagnostic agreement between different clinicians has been shown to be poor; vaginal pain and spasms did not differentiate between women with vaginismus and dyspareunia (a genital pain disorder; i.e. painful sex) resulting from vulvar vestibulitis (Reissing et al., 2004) In addition, many of the health professionals usually involved in the assessment of vaginismus have insufficient expertise in diagnosing the muscular spasm, not to mention there being a lack of consensus around which muscles are involved in the spasms. Furthermore, it is difficult to discern whether the vaginal spasms have developed as a defense to painful attempts, or whether the spasms are what cause the pain. Some women with vaginismus display similar characteristics as people with specific phobias (hence why I sometimes use the term vaginal penetration phobia) (Lahaie et al., 2010). Fear of pain is the primary reason for some women with vaginismus abstaining from and avoiding sex, and so the previous classification of vaginismus does not take enough into account how fear plays into its development.
These are some of the reasons why the new version of the DSM (fifth edition) combined vaginismus, dyspareunia, and other penetration disorders into one main and broader diagnosis: genito-pelvic pain/penetration disorders (GPPPD) (American Psychiatric Association, 2013). The new DSM-V guidelines specify that if the woman has recurrent and distressing difficulty with one (or more) of the following for at least six months, then a GPPPD diagnosis is warranted:
- vaginal penetration during intercourse
- marked vulvovaginal or pelvic pain during intercourse or attempted intercourse
- marked fear or anxiety about the experience of vaginal or pelvic pain as related to vaginal penetration
- marked tensing of the pelvic floor muscles during attempted vaginal penetration
(Perez & Binik, 2016)
I should note that, though the diagnoses of vaginismus, dyspareunia, and other penetration difficulties have been merged into GPPPD, the treatment guideline I describe in this book is mostly based on my work with women who suffered from either vaginismus or vaginal penetration phobia (which, together, I will refer to as “penetration disorders” throughout the book), and not dyspareunia. And so though many of the suggestions in this book could also be beneficial in treating painful sex, it must be noted that they may not be appropriate or sufficient for some of these cases. I may use the terms GPPPD, vaginismus, or penetration disorders interchangeably throughout the book to refer to the condition. If PIV sex or attempted vaginal penetrative sex is painful, it may be useful for the client to consult a pelvic physical therapist (if they are available where the client resides) for a complete evaluation to assess whether there may be organic or physical causes for the pain. If the client has no access to a physical therapist specializing in pelvic issues, then they may consult a qualified gynecologist instead.
Prior to the development of the GPPPD diagnosis in the DSM-V, I personally did not rely solely on identifying muscular spasms for the diagnosis of vaginismus. Whenever a client presented to me with a self-report of either not being able to have PIV sex, complete a gynecological exam, or insert a tampon, I would treat the condition in a similar manner. My preferred definition has thus been inspired by Basson et al. (2004) who recommend the following guidelines:
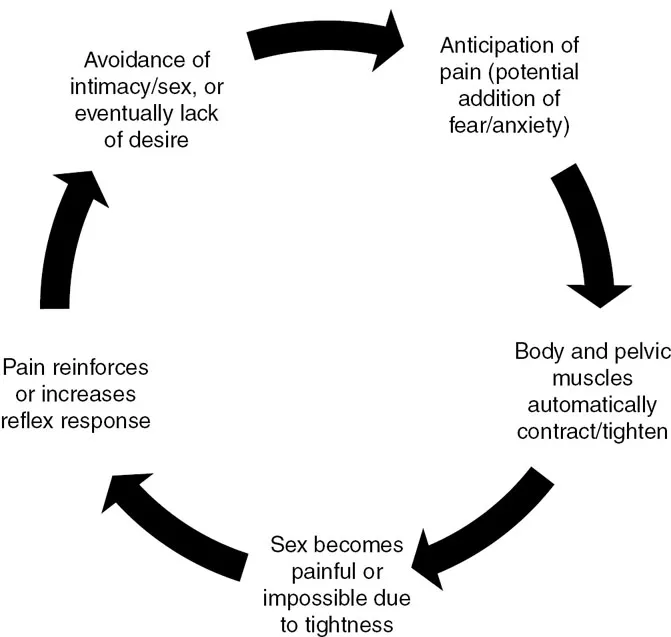
So to put it simply, if a woman is unable to have vaginal penetrative sex or insert a tampon or have a gynecological exam due to either fear or uncontrollable muscle contractions, despite her desire to do so, and this difficulty is causing her distress, then I would approach it similarly to treating vaginismus, with a great focus on her fears and discomfort. Even if she is not experiencing muscle contractions and is merely experiencing an uncontrollable phobic response or avoidance (specific phobia linked to sex or vaginal penetration), I would follow the same guidelines. In other words, one way in which GPPPD may show up is that the couple may be attempting vaginal penetrative sex and the penis might not be able to enter the vagina because there is a tightening/tensing of her vaginal and pelvic muscles, or because of pain. Alternatively, the couple may not actually be having any penile-vaginal contact and they are unable to have PIV sex because of the woman’s avoidance behaviors such as tightening and closing of the legs, pushing the partner away, or moving away from the partner. In both situations there is an experience or anticipation of pain and/or vaginal penetration, and in my opinion, it is that experience or fear that is underlying vaginismus or dyspareunia in many women (Leiblum, 2007, p. 125). Though the treatment plans in both cases generally look the same in my approach, they will and should, of course, be tailored to each individual according to her needs, circumstances, and severity. Therefore, this book offers a general guide to overcoming this difficulty, which I encourage the reader to modify according to what they deem would be best for their client or situation.
Vaginismus may arise as part of a conditioning response that is acquired secondarily to negative physical and/or psychological stimuli. This means that a woman can associate sex or any other penetrative activity with physical pain, fear, or trauma, if she experienced one (or more) incident(s) where the physical or psychological stimuli were present at the same time as a sexual or genital experience. It is one of the most common female sexual dysfunctions – prevalence rate is not accurately known and varies in different parts of the world (figures range from 5 percent to 43 percent depending on where the data was collected and how it has been classified, and tends to be higher in Muslim-populated countries) (Oksuz & Malhan, 2006; Perez, Brown, & Binik, 2016; Nobre, Pinto-Gouveia, & Gomez, 2006; Laumann, Paik, & Rosen, 1999; Lau, Kim, & Tsui, 2005; Leiblum, 2007, p. 130). I can confidently say that it was the most common presenting issue Arab and South-Asian women would bring to me in therapy during my years practicing in the UAE, which supports some of the evidence that it tends to be more common in more conservative and religious parts of the world.
What Is Dyspareunia?
Though this book is not about dyspareunia specifically, I am going to briefly describe it, as some women suffer from it in addition to vaginismus and separating the two can get confusing. As vaginismus and dyspareunia can be a common comorbidity (co-occurring diagnoses), it is likely that this is one of the reasons they have been merged into one main category. Put simply, dyspareunia is recurrent genital pain associated with sexual activity (could be superficial/external, vaginal, or deep). It is usually used to describe pain on penetration but can occur during genital stimulation. In situations where dyspareunia is an issue, I highly recommend stopping any activity that is painful, and consulting a gynecologist or pelvic physical therapist to check for any potential physical abnormality, or medical/organic cause such as infection, inflammation, endometriosis, or cysts.
If no medical cause is found, it is often a result of insufficient lubrication and/or low arousal, which generally happens if the woman is not relaxed (such as if she has vaginismus or is anxious/fearful), and/or is not excited enough (for example, if she has low desire, or is not attracted to the partner, or is anxious, or not stimulated in the appropriate manner). At times paying more attention to sensual touch and appropriate sexual stimulation helps, if it is mainly a matter of creating more arousal. And sometimes couples therapy may be advised if problems in the relationship are leading to a lack of interest in or aversion to sex. Though this book discusses the integrated treatment of penetration disorders, which are part of GPPPD, I cannot claim that it can also treat painful sex, as there could be other potential factors involved in pain. What I can say, however, is that incorporating some of the themes or exercises provided in this book could potentially be helpful in addressing the pain, depending on the specific case and causes.