This long-awaited new edition of the author's seminal text on orthognathic surgery includes not only a fresh new look and over a dozen new cases, but essential updates for anyone practicing orthognathic surgery. Though many of the surgical practices and techniques have not drastically changed since the previous edition, recent research has inspried new sections on airway management and orthoganthic surgery of the tempormandibular joint. The previous chapter on treatment of dentofacial deformities has now been split into two streamlined chapters on typical and complex dentofacial deformities to accommodate new cases and information, allowing a more user-friendly experience for the reader. Those familiar with the second edition will remember the illustrated step-by-step processes for patient evaluation, diagnosis, treatment planning, and surgical technqiue, and these vital resources have made it to the new text as well. From the most basic bilateral sagittal split osteotomy to complex surgery involving three-dimensional analysis, movement, and rotation of both jaws, this book will help everyone from surgical residents to experienced clinicians in managing both children and adults with dentofacial deformities, improving both function and esthetics.
- 320 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
When people recognize malpositioned teeth or obvious jaw deformities, they usually seek treatment from an orthodontist, who can improve tooth alignment, function, and facial esthetics. More severe deformities that require a combination of orthodontics and surgery for correction are called dentofacial deformities. These deformities can affect physical orofacial function in several ways. Mastication can be impaired, and—especially in severe cases—this impairment can affect digestion and general nutritional health. Lip incompetence due to excessive vertical growth of the maxilla results in mouth breathing, which eliminates the physiologic effect of the nose on breathing. Speech is often affected by dentofacial deformities despite the body’s adaptive capabilities. Malpositioned teeth may have a profound effect on proper oral hygiene maintenance, making teeth more susceptible to dental caries and periodontal disease. The patency of the airway and normal breathing is certainly affected by the position of the jaws, and dentofacial deformities are currently considered an important etiologic factor in the development of obstructive sleep apnea. Several types of dentofacial deformities also affect temporomandibular function. The physical effects of a dentofacial deformity are important, but the psychosocial impact of a dentofacial deformity on an individual is often paramount. This type of deformity can profoundly affect the quality of life and may entail lifelong adjustment.
Treatment Options for Dentofacial Deformities
The combination of surgery and orthodontic treatment makes it possible to treat dentofacial deformities that are not possible to correct with orthodontics alone (eg, vertical maxillary excess and severe anterior open bite malocclusion). Orthognathic surgery has created new and exciting opportunities in the treatment of patients with dentofacial deformities and provided the orthodontist with options other than compromised treatment for patients with skeletal disharmony. Experience in orthognathic surgery, an increased understanding of its biologic basis, and a refinement of its art form now enable us to routinely deliver a stable, esthetic, and functional result to patients. When severe skeletal discrepancies result in malocclusion, three kinds of treatment are available: growth modification, orthodontic camouflage, and orthognathic surgery.
Growth modification
This treatment approach should only be considered for mild skeletal deformities. In growing children, dentofacial orthopedics can alter the expression of growth to some extent. However, the extent of growth alteration varies, and this topic remains controversial. The following facial growth patterns may be influenced by growth modification in adolescents:
- Maxillary anteroposterior excess: Excessive horizontal growth of the maxilla may be impeded by headgear or camouflaged by extraction of the maxillary first premolars and orthodontic retraction of the incisors.
- Maxillary anteroposterior deficiency: Moderate improvement can be established by orthodontic protraction.
- Vertical maxillary excess: High-pull headgear with temporary anchorage devices can impede the vertical growth of the maxilla and diminish the severity of the deformity.
- Mandibular anteroposterior deficiency: Headgear combined with functional appliances may improve mandibular projection.
Skeletal deformities such as mandibular anteroposterior excess, vertical maxillary deficiency, and microgenia cannot be easily influenced by growth modification. In addition, there are some patients who may undergo growth modification for a long period of time with headgear or elastics and end up still requiring a surgical approach. This can be very disappointing and frustrating for the patient as well as their family and health care providers.
Preparing for surgery in these cases would often also require “reverse” orthodontics, decompensating the attempts to compenstate the dentition before orthognathic surgery, prolonging treatment even further.
Orthodontic camouflage
Certain patients with mild skeletal discrepancies would benefit from orthodontic camouflage rather than surgery. Dental compensation for a skeletal deformity, or orthodontic camouflage, may, however, be associated with impaired esthetics, questionable posttreatment stability, and prolonged treatment time (see Figs 1-2 and 1-3). Corrective treatment may require rebanding and a second orthodontic treatment followed by orthognathic surgery.
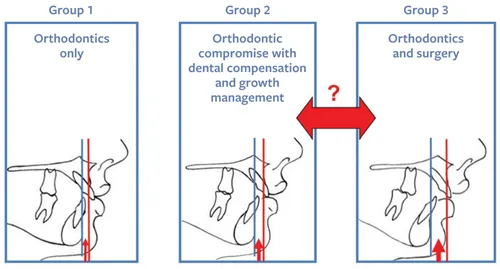
Fig 1-1 Patients who may seek treatment for their malocclusions from an orthodontist can in general be divided into three categories according to the severity of their skeletal deformities. When planning treatment, it can be challenging but is essential to differentiate between groups 2 and 3.
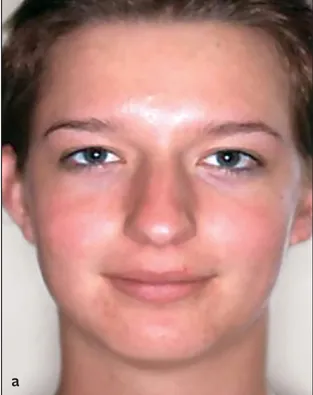





Fig 1-2 (a to f) A 19-year-old patient with a skeletal Class II relationship who would be considered to fall into group 3. Her maxillary first premolars were removed and the maxillary incisors retracted in an attempt to correct her occlusion. Unfortunately, the treatment compromised her esthetics and occlusion, resulting in a severe convex profile that accentuated her prominent nose and a Class II deep bite malocclusion.
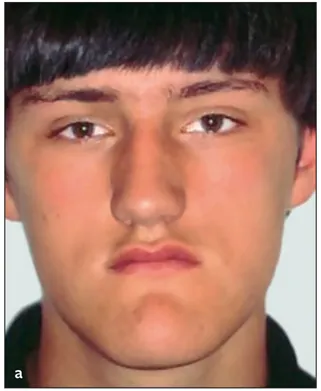
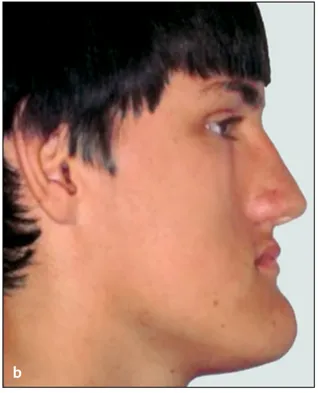

Fig 1-3 (a to c) A 16-year-old patient with a skeletal Class III relationship. His four premolars were removed at a younger age, and an attempt was made to establish an occlusion with orthodontic treatment. This is an example of a patient that would fall into the group 3 category; however, he was treated with orthodontics only.
Orthognathic surgery
Combined orthodontic and surgical correction is considered the best treatment modality for dentoskeletal imbalances once growth has ceased. Although orthognathic surgery is associated with certain risks and challenges, it has become a more refined and less traumatic procedure for patients and therefore is now a reasonable treatment option. Improving skeletal relationships will result in remarkable facial changes, and this is an important goal to consider.
Selecting a treatment
Patients seeking orthodontic treatment have a wide range of functional and esthetic needs and can be divided into three groups (Fig 1-1):
- Group 1: Those with a normal skeletal relationship and malocclusions that can be treated using routine orthodontic techniques.
- Group 2: Those with mild to moderate skeletal discrepancies. The malocclusions of many of the patients in this group can be corrected by dental compensation and growth management. Both options—pursuing only orthodontic treatment and pursuing combined treatment—will have advantages and disadvantages that must be discussed between the clinicians, the patient, and the patient’s parents (if necessary). There are several factors that will determine the treatment decision.
- Group 3: Those with moderate to severe skeletal discrepancy and noticeable facial imbalance. The negative effects of compromised orthodontic treatment for patients in the third group would be unacceptable, making combined surgery and orthodontics the treatment of choice. In cases when the surgical option is not acceptable to the patient, it would be wise for the surgeon not to accept the patient for treatment. Orthodontic treatment alone for patients in this group will certainly worsen the esthetics, have doubtful stability, and possibly have negative long-term periodontic implications (Figs 1-2 and 1-3). On the other hand, only pursuing surgery without orthodontics would also lead to compromise.
An important challenge for the clinician is to differentiate between patients on the borderline between group 2 and group 3. An orthodontic camouflage treatment for patients in group 3 would be a mistake, just as surgical treatment of certain patients in group 2 would be inappropriate. The decision regarding the best treatment for borderline patients is influenced by various factors:
- The patient’s main complaint and preferences. Some patients are interested only in improving occlusion, whereas esthetic change is a high priority for others. The patient’s priority is an important factor in treatment planning: The patient needs to be able to weigh the two treatment options against each other and must therefore be well informed.
- Long orthodontic treatment. This often involves headgear, functional appliances, and a different extraction pattern with a compromised treatment outcome. The possibility of worsening esthetics, instability, and long-term periodontal problems should be discussed with the patient (and parents when applicable).
- Shorter orthodontic treatment combined with surgery. The surgical implications, possible complications, and improved treatment outcome must be discussed with the patient (and parents when applicable).
- The orthodontist’s preferences and skills. If the orthodontist has encountered poor surgical results with previous patients, there will be a natural hesitation to continue to recommend surgery. The orthodontist’s confidence in the success of surgery is an important factor.
- Available surgical skills. Orthognathic surgical expertise may ...
Table of contents
- Cover
- Title page
- Copyright page
- Contents
- Preface
- 1 Principles of Orthognathic Surgery
- 2 Systematic Patient Evaluation
- 3 Diagnosis and Treatment Planning
- 4 Diagnosis and Treatment of Typical Dentofacial Deformities
- 5 Diagnosis and Treatment of Complex Dentofacial Deformities
- 6 Surgical Technique
- Index
- Back Cover
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Essentials of Orthognathic Surgery by Johan P. Reyneke in PDF and/or ePUB format, as well as other popular books in Medicine & Dentistry. We have over 1.5 million books available in our catalogue for you to explore.