
Essentials of Orthognathic Surgery
Third Edition
Johan P. Reyneke
- 320 pagine
- English
- ePUB (disponibile sull'app)
- Disponibile su iOS e Android
Essentials of Orthognathic Surgery
Third Edition
Johan P. Reyneke
Informazioni sul libro
This long-awaited new edition of the author's seminal text on orthognathic surgery includes not only a fresh new look and over a dozen new cases, but essential updates for anyone practicing orthognathic surgery. Though many of the surgical practices and techniques have not drastically changed since the previous edition, recent research has inspried new sections on airway management and orthoganthic surgery of the tempormandibular joint. The previous chapter on treatment of dentofacial deformities has now been split into two streamlined chapters on typical and complex dentofacial deformities to accommodate new cases and information, allowing a more user-friendly experience for the reader. Those familiar with the second edition will remember the illustrated step-by-step processes for patient evaluation, diagnosis, treatment planning, and surgical technqiue, and these vital resources have made it to the new text as well. From the most basic bilateral sagittal split osteotomy to complex surgery involving three-dimensional analysis, movement, and rotation of both jaws, this book will help everyone from surgical residents to experienced clinicians in managing both children and adults with dentofacial deformities, improving both function and esthetics.
Domande frequenti
Informazioni
- Maxillary anteroposterior excess: Excessive horizontal growth of the maxilla may be impeded by headgear or camouflaged by extraction of the maxillary first premolars and orthodontic retraction of the incisors.
- Maxillary anteroposterior deficiency: Moderate improvement can be established by orthodontic protraction.
- Vertical maxillary excess: High-pull headgear with temporary anchorage devices can impede the vertical growth of the maxilla and diminish the severity of the deformity.
- Mandibular anteroposterior deficiency: Headgear combined with functional appliances may improve mandibular projection.
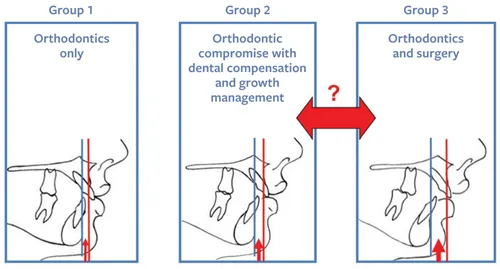






- Group 1: Those with a normal skeletal relationship and malocclusions that can be treated using routine orthodontic techniques.
- Group 2: Those with mild to moderate skeletal discrepancies. The malocclusions of many of the patients in this group can be corrected by dental compensation and growth management. Both options—pursuing only orthodontic treatment and pursuing combined treatment—will have advantages and disadvantages that must be discussed between the clinicians, the patient, and the patient’s parents (if necessary). There are several factors that will determine the treatment decision.
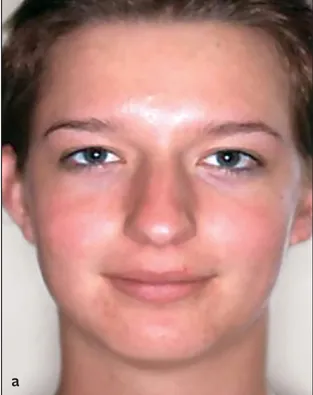
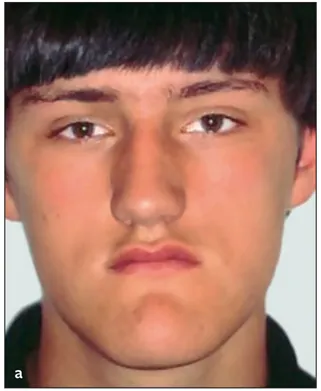
- Group 3: Those with moderate to severe skeletal discrepancy and noticeable facial imbalance. The negative effects of compromised orthodontic treatment for patients in the third group would be unacceptable, making combined surgery and orthodontics the treatment of choice. In cases when the surgical option is not acceptable to the patient, it would be wise for the surgeon not to accept the patient for treatment. Orthodontic treatment alone for patients in this group will certainly worsen the esthetics, have doubtful stability, and possibly have negative long-term periodontic implications (Figs 1-2 and 1-3). On the other hand, only pursuing surgery without orthodontics would also lead to compromise.
- The patient’s main complaint and preferences. Some patients are interested only in improving occlusion, whereas esthetic change is a high priority for others. The patient’s priority is an important factor in treatment planning: The patient needs to be able to weigh the two treatment options against each other and must therefore be well informed.
- Long orthodontic treatment. This often involves headgear, functional appliances, and a different extraction pattern with a compromised treatment outcome. The possibility of worsening esthetics, instability, and long-term periodontal problems should be discussed with the patient (and parents when applicable).
- Shorter orthodontic treatment combined with surgery. The surgical implications, possible complications, and improved treatment outcome must be discussed with the patient (and parents when applicable).
- The orthodontist’s preferences and skills. If the orthodontist has encountered poor surgical results with previous patients, there will be a natural hesitation to continue to recommend surgery. The orthodontist’s confidence in the success of surgery is an important factor.
- Available surgical skills. Orthognathic surgical expertise may ...