Among neurodegenerative diseases, those that lead to a state ofdementia are the aim of severalinvestigations. Dementia is a chronic disease the prevalence of whichis increasing worldwide. Thenumber of dementia patients in the world is approximately 50 million, and it is estimated that thenumber of patients will reach 131.5 million by 2050. This increase willbe accompanied by asignificant increase in medical expenditures and other expenses, especially for elderly patients.Therefore, the maintenance cost of dementia in the future is expectedto be quite high. For thisreason, several investigations aim, firstly, to describe the keymechanisms involved in the originof dementia and, secondly, to establish preventive and therapeuticstrategies in order tounderstand and mitigate this debilitating pathology. This volume of Frontiers in Clinical Drug Research -Dementia explores the current comorbidities that cause cognitiveimpairment and the current management alternatives for clinical cases ofdementia. The reviews contributed in these volume will provide readers with acurrent perspective on the subject. The topics covered in this volume include: - Comorbidities inducing mild cognitive impairment - an evaluation ofthe risk caused by some pathological conditions- Tau-targeted therapy in Alzheimer's disease - history and currentstate- Emerging nanotherapeutic strategies in Alzheimer's disease- Implication of dehydroepiandrosterone on dementia related tooxidative stress- Polyphenol compounds as potential therapeutic agents in Alzheimer'sdisease The volume is a timely update on dementia treatment for clinicalphysicians, neurologists, gerontologists, pharmaceutical and medicinal chemistryresearchers, and physiologists.
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Frontiers in Clinical Drug Research - Dementia
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
Scienze fisicheSubtopic
Chimica clinicaTau-Targeted Therapy in Alzheimer's Disease - History and Current State
Anamaria Jurcau1, *, Vharoon Sharma Nunkoo1
1 University of Oradea, Faculty of Medicine and Pharmacy, Clinical Municipal Hospital, Dr. G. Curteanu”, Oradea, Romania
Abstract
The two main histopathological hallmarks still required for the diagnosis of Alzheimer's disease are the presence of amyloid plaques and intraneuronal neurofibrillary tangles formed mainly of tau protein. Normally, tau protein regulates intracellular trafficking and provides microtubule stability. However, in AD as well as in other tauopathies, there is a disruption in the normal function of tau, leading to the development of neurofibrillary tangles with disease-dependent ultrastructure of the tau filaments.
After several failures of trials with drugs trying to prevent the accumulation of amyloid, tau protein became another target of molecules designed to modify the course of AD.
Each stage in the development of tau pathology, from the expression of tau protein to its post-translational modifications, with the protein’s aggregation and impaired clearance, presents opportunities for therapeutic intervention: reducing tau expression with antisense oligonucleotides, reducing tau phosphorylation with kinase inhibitors, inhibiting tau acetylation, tau deglycosylation, tau aggregation, modulating tau degradation, stabilizing the microtubules, as well as active or passive anti-tau immunotherapies (with various monoclonal antibodies), have been attempted or are still in trials, with rather inconclusive results so far. It appears that an efficient disease-modifying therapy is not yet available. Given the complex pathophysiology of Alzheimer’s disease, most likely, a multi-targeted approach would be more effective.
Keywords: Alzheimer’s disease, Anti-tau therapy, Microtubules, Mitochondrial dysfunction, Tauopathies, Tau protein.
* Corresponding author Anamaria Jurcau: The University of Oradea, Faculty of Medicine and Pharmacy, Oradea, Romania; E-mail:[email protected]
HISTORICAL BACKGROUND
Alois Alzheimer, a German physician and a pioneer of linking disease symptoms to microscopic brain changes, first met and examined Auguste D. in 1901 in Frankfurt. Although 1 year later he took a position in Munich, he was haunted by this case. Thus, in April 1906, when the patient died, he examined her brain and found impressive shrinkage and abnormal depositions in and around nerve cells. Today, more than 100 years after the presentation of Alzheimer's findings at the Conference held in Tübingen in November 1906 [1, 2], amyloid plaques and neurofibrillary tangles are still required for the pathological diagnosis of Alzheimer's disease [3].
Using the newly discovered electron microscopy technique, Terry and Kidd described the intraneuronal deposits in 1963 as being paired helical filaments [4, 5]. Further, in 1975, Weingarten and coworkers characterized these filaments as being a protein named tau, which is crucial for the assembly of tubulin into microtubules [6]. Interestingly, 1975 was the same year in which tau the lepton was also discovered by Perl et al. [7]. Soon thereafter, Cleveland and coworkers provided a biochemical characterization of tau [8, 9].
However, because monogenic mutations in the amyloid precursor protein (APP) or the presenilins involved in its processing can lead to phenotypes similar to AD, until recent years, research has focused mainly on these molecules. The discovery of tau mutations able to cause neurodegenerative diseases on their own [10] as well as of intracellular tau aggregates in several neurodegenerative diseases like progressive supranuclear palsy, frontotemporal lobar degeneration, corticobasal degeneration, or Pick's disease (collectively referred to as tauopathies) [11], boosted tau research and led to exploring several therapeutic strategies in neurodegenerative diseases [7, 12, 13].
NORMAL TAU PROTEIN STRUCTURE AND FUNCTION
The Tau Gene and Tau Isoforms
Human tau is encoded by the MAPT (microtubule-associated protein tau) gene located on chromosome 17q21 [14]. Alternative splicing generates mainly 6 isoforms of 37-46 kDa in the central nervous system (CNS), while a “big tau” isoform is found mainly in the peripheral nervous system [15, 16]. The six isoforms found in the CNS (Fig. 1) differ by the presence of zero, one, or two N-terminal inserts and either 3 (3R) or 4 (4R) microtubule binding C-terminal inserts
[17]. Due to the developmentally regulated expression of tau, all 6 isoforms can be found in the adult human brain, while the fetal brain expresses only the shortest isoform (0N3R) [18].
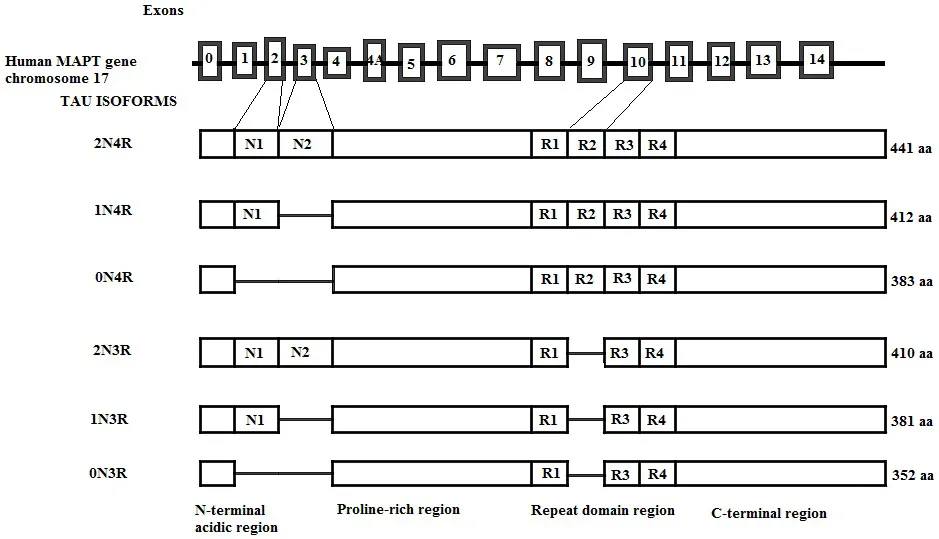
Genomic structure of the human tau gene; of the 14 exons, exons 2, 3, and 10 are alternatively spliced, generating six tau isoforms in the adult brain. Exons 9, 11, and 12 each encode for a microtubule-binding repeat generating 3R tau isoforms. The presence of E10 adds an extra MT-binding repeat generating 4R tau isoforms. 3R and 4R tau isoforms further differ depending on the presence of exon 2 (1N) or exons 2 and 3 together (2N), while the absence of both exons generates 0N3R and 0N4R isoforms of tau. The number of aminoacids in each isoform is shown on the right.
Tau Protein Structure
The amino acid composition of tau is unusually hydrophilic [19], and the protein has an overall basic character. The charges have an asymmetrical distribution, with the amino-terminal being acidic and the carboxy-terminal being neutral. The middle region contains numerous prolines which harbor many epitopes of antibodies that are hyperphosphorylated in Alzheimer's disease [12].
Due to its hydrophilic character, the polypeptide chain of the protein is flexible and mobile. Tau is normally unfolded as opposed to most cytosolic proteins, which have a compact folded structure [20, 21]. To date, the “paperclip” conformation of tau is widely accepted, in which the C-terminus is folded over the microtubule-binding domain, and the N-terminus folds over the C-terminus [22], as shown in Fig. (2). This conformation is disrupted by tau phosphorylation [9].

In the free tau folded into the paperclip conformation, the C-terminal domain lies close to the N-terminus and protects the domain comprising aminoacids 2-18, known as the phosphatase activating domain to interact with protein phosphatase 1 (PP1). When the C-terminal domain moves away from the N-terminal domain, the phosphatase activating domain activates PP1, which activates further glycogen synthase kinase 3β (GSK3β) and initiates the phosphorylation cascade.
Tau Localization
Tau Localization in Neurons
Tau is located mainly in axons [23] but can be found in lower concentrations in the plasma membrane, nucleus, mitochondria, as well as in dendrites and at the level of synapses [24].
Multiple mechanisms that contribute to the predominantly axonal localization of tau are as follows: - cytosolic tau diffuses freely between the different compartments but is retained in the axon through its binding to microtubules favored by the low phosphorylation level and the retrograde barrier formed by the initial segment of the axon, which “traps” tau in the axon [25].
- tau is transported actively by motor pr...
Table of contents
- Welcome
- Table of Content
- Title
- BENTHAM SCIENCE PUBLISHERS LTD.
- Preface
- List of Contributors
- Comorbidities Inducing Mild Cognitive Impairment, an Evaluation of the Risk Caused by some Pathological Conditions
- Tau-Targeted Therapy in Alzheimer's Disease - History and Current State
- Implication of Dehydroepiandrosterone on Dementia Related to Oxidative Stress
- Emerging Nanotherapeutic Strategies in Alzheimer's Disease
- Polyphenol Compounds as Potential Therapeutic Agents in Alzheimer’s Disease
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Frontiers in Clinical Drug Research - Dementia by José Juan Antonio Ibarra Arias in PDF and/or ePUB format, as well as other popular books in Scienze fisiche & Chimica clinica. We have over 1.5 million books available in our catalogue for you to explore.