This concise handbook has a unique approach and covers all important aspects of head and neck cancers from basic topics like carcinogenesis to advanced treatment options such as immunotherapy, electrochemotherapy, and robotic surgery in a succinct way. As every treatment center manages its patients with a different modality as per their institutional protocol, this book endeavors to standardize the processes by discussing the management of cancers of all anatomic areas in view of the National Comprehensive Cancer Network (NCCN) guidelines, which is the committee that prepares protocols for management of cancers and every head and which neck oncosurgeons must adhere to for their clinical practice.
Key Features
Explains the topics through flowcharts and diagrammatic representations that are helpful for exam preparation
This book aims to serve as a valuable resource for postgraduate residents of maxillofacial surgery, ENT and otolaryngology, general surgery, plastic surgery, and junior specialists
Serves as a comprehensive, evidence-based quick reference for the clinician on the go
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Carcinogenesis is the process of induction of tumor and the agents that induce these tumors are called carcinogens. Carcinogens are broadly classified into
Chemical carcinogens
Physical carcinogens
Hormonal carcinogens
Biological carcinogens
Chemical Carcinogens
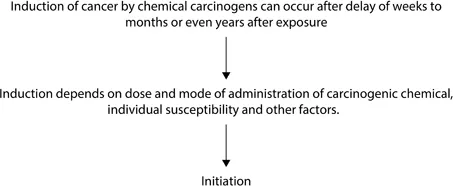
The first report of any chemical-causing neoplasia came from the observation in 1775 that there was a higher incidence of scrotum cancer in chimney sweepers in London than in the general population (Flowcharts 1.1 and 1.2).
Flowchart1.1Initiation of carcinogenesis.
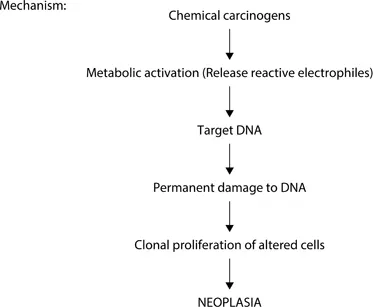
Flowchart1.2Mechanism of carcinogenesis.
A single dose of an initiating agent for a large duration is more effective than a short dose with frequent exposure:
UV light: The main source of UV radiation is sunlight. It usually penetrates the skin for a few millimeters so that its effect is limited to epidermis. Excessive exposure can cause various forms of skin cancers, such as basal cell carcinoma, keratoacanthoma, and malignant melanoma.
Ionizing radiation: This includes all kinds such as X-rays, radioactive isotopes, protons, and neutrons. The most frequent radiation-induced cancers are leukemia, thyroid cancers, skin cancers, and salivary gland tumors.
Hormonal Carcinogenesis
Cancer is more often seen to develop in organs that undergo proliferation under the influence of excessive stimulation of hormones. Hormone-sensitive tissues that develop tumors are the breast, endometrium, vagina, prostate, and testis.
Biological Carcinogenesis
Biological carcinogenesis has been studied that about 20% of all cancers worldwide are viral-associated cancers. Sanarelli, an Italian physician, in 1889 was the first person who observed the association of oncogenic viruses with the neoplasia.
Examples include DNA oncovirus: Human papillomavirus/Epstein-Barr virus/cytomegalovirus/herpes simplex virus. RNA oncovirus: Human T-cell lymphotropic virus (HTLV).
Theories of Carcinogenesis
Important information:
Proto-oncogenes: These are normal genes that bring about cellular differentiation and growth. They can be converted into oncogenes.
Oncogenes: These are genes associated with neoplastic transformation.
Anti-oncogenes: These are cells that normally suppress cell proliferation. They are also called tumor suppressor genes.
Cancer may arise not only by activation of proto-oncogenes into oncogenes but also by suppressor of anti-oncogenes.
The following sections discuss the theories of carcinogenesis.
Genetic Theory
Genetic theory is the most popular and accepted theory. This theory suggests that the cells become neoplastic due to alterations in the DNA. The mutated cell transmits its character to the next progeny.
Epigenetic Theory
According to epigenetic theory, carcinogenic agents act on the activators or suppressors of genes and not on the gene themselves, which results in the abnormal expression of genes.
Multistep Theory
Carcinogenesis is a multistep process. This is substantiated by in vitro changes in the experimental animals as well as in vivo changes in human cancers.
For example, in chemical carcinogenesis, two essential features occur in proper sequence—initiation and promotion.
Most cancers arise after several mutations, which have been acquired in proper sequential manner.
Immune Surveillance Theory
An immune-competent host often mounts an attack on developing tumor cells to destroy them, while an immune incompetent host fails to destroy them. Some evidence in support of this theory is the fact that there is a high incidence of cancer in AIDS patients and most cancers occur in old people, where the host immune response is weak.
Monoclonal Theory
This theory suggests that cancers arise from a single clone of transformed cells.
Tumor Heterogeneity
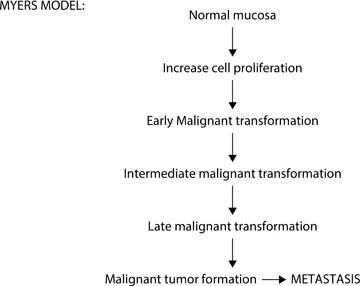
This theory by Fidler and Ellis1 states that a tumor is composed of subpopulations heterogeneous of cells. They will differ with respect to their immunogenicity, invasiveness, and sensitivity to cytotoxic drugs. But the environment of local tumor cells may favor the expansion of more aggressive clone information of metastasis (Flowcharts 1.3 and 1.4).
Flowchart1.3Myers model.
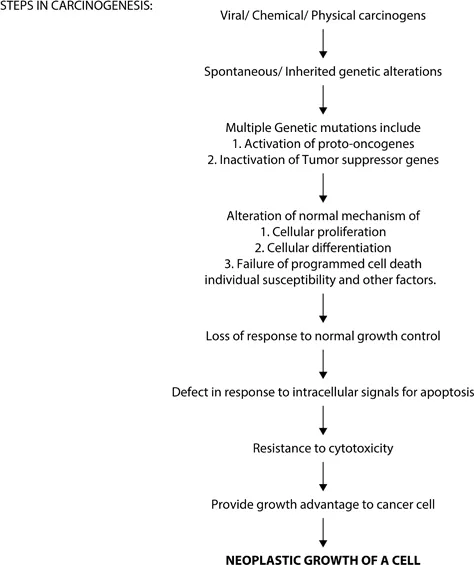
Flowchart1.4Steps in carcinogenesis.
Field Cancerization
Secondary tumors of the oral cavity have a sobering effect on the prognosis for head and neck cancer (HNC) patients. These tumors are most often seen to develop in the oral cavity but can also be seen in lungs or esophagus from which 10–40% of patients with HNC are often fatal. One of the reasons for this multifocal tumor origin was proposed around 40 years ago by Slaughter et al. In accordance with his concept of field cancerization, there are multiple cell groups that independently undergo neoplastic transformation due to stress of regional carcinogenic activity. There are certain molecular genetic approaches that have been recently challenged with the fact that independent transforming events are more common in the epithelial mucosa of HNC patients. Often, when a primary cancer is compared with a secondary tumor somewhere in oral cavity/upper aerodigestive tract, these paired tumors often harbor cells that have identical patterns of genetic alterations or mutations. It is assumed that single cell regimens a critical genetic for advantage of growth over its neighboring cells. At some point of time after the transformation, cells which harbor these early genetic alterations then migrate to nearby adjacent areas to populate contiguous tracts of mucosa further accumulating other alterations that later acquire additional growth advantages from the surrounding environment, and ultimately transform into aggressive subclones that may be separated by space and time.
Secondly, collective observations have supported the view that the epithelial mucosa of the upper aerodigestive tract may become populated by these genetically damaged clones of cells, which may lack any histopathological evidence of dysplastic features. The presence of these genetically damaged but morphologically intact cells not only explains the phenomenon of fi...
Table of contents
Cover Page
Half-Title Page
Title Page
Copyright Page
Dedication Page
Contents
Foreword by Jatin P. Shah
Foreword by Ashok R. Shaha
A Note from the Editor
Preface
Acknowledgments
1 Carcinogenesis
2 Molecular Biology of Cancer and Biomarkers
3 TNM Staging and Grading
4 Lymphatic System and Lymph Nodes
5 Imaging
6 Sentinel Node Biopsies (SNBs)
7 Histopathological Parameters for Prognosis of Disease
8 Clinical Assessment of Head and Neck Cancer Patients
9 Management of the Neck
10 Access Osteotomies
11 Oral Cavity and Lips
12 Pharynx
13 Larynx
14 Paranasal Sinuses
15 Salivary Glands
16 Thyroid Gland
17 Orbit and Eyelids
18 Occult Primary
19 Management of Carotid Blowout
20 Chemotherapy
21 Radiotherapy
22 Electrochemotherapy
23 Targeted Therapy, Immunotherapy, and Gene Therapy
24 Robotic Surgery of Head and Neck Cancers
25 Perioperative Management of Head and Neck Cancer Patients
26 Pain Management of Locally Advanced Head and Neck Carcinomas/Palliative Care Patients
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Head and Neck Oncology by Akheel Mohammad,Ashmi Wadhwania,Mohammad Akheel in PDF and/or ePUB format, as well as other popular books in Medicine & Ear, Nose & Throat Medicine. We have over 1.5 million books available in our catalogue for you to explore.