The book is intended as a concise overview of current orthopaedic practice. It will be of interest to orthopaedic surgeons in practice and to orthopaedic trainees - both specialist and basic surgical, in particular, orthopaedic specialist registrars in the UK preparing for the FRCS Orth. exam, or trainees in other countries at an equivalent stage of orthopaedic training. Medical students doing orthopaedic attachments will find it a practical reference tool. In addition, individuals involved in the care of orthopaedic patients, such as physiotherapists and nurse practitioners, will find the book useful. With increasing subspecialisation in orthopaedic surgery, it is more difficult for the specialist to keep abreast of recent changes and current trends in the management of orthopaedic conditions other than their own area of interest. This book aims to fill that void and will be an easily readable source with information that is concise and current. Emphasis is placed on the current literature and an effort has been made to provide evidence on controversial topics with annotated references incorporated into the text. These will be a useful resource for further reading. Any reader wishing to gain insight into 21st century orthopaedic surgery will find this book of interest and value.
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineChapter 1 Arthroplasty
Total hip replacement
Total hip replacement (THR) is one of the most successful operative procedures in orthopaedic surgery.
Indications
The indications for THR are as follows:
•To relieve hip pain that is unresponsive to non-operative measures.
•To improve function.
The vast majority of hip replacements are performed because of osteoarthritis. Other indications include rheumatoid arthritis, post-traumatic arthritis, avascular necrosis, dysplastic hip in skeletally mature patients, failed fracture fixations and tumours.
There is an increasing trend towards THR in active patients of 50-80 years with displaced femoral neck fractures.
Contraindications
Contraindications to THR include the following:
•Active infection in the hip.
•Relative contraindications include poor abductor function, medical condition or mobility, an immature skeleton and progressive neurologic disease.
Note
Blomfeldt R, Törnkvist H, Ponzer S, et al. Comparison of internal fixation with total hip replacement for displaced femoral neck fractures. Randomised, controlled trial performed at four years. J Bone Joint Surg Am 2005; 87: 1680-8. This study looked at 102 patients with a femoral neck fracture. All were older than 70 years and had intact cognitive function. At 4 years, the mortality rate was 25% in both the internal fixation and THR groups. The THR group had a 4% complication and 4% reoperation rate. The fixation group had a 42% complication rate and 47% reoperation rate. Hip function was better in the THR group.
Assessment and investigations
Pre-operative assessment should include the following:
•A detailed history and examination to confirm that the hip joint is the source of pain.
•Full blood count, electrolytes and urine analysis to check for urinary tract infection.
•Nasal and perineal swabs for MRSA.
•Cross-matching (or autodonation) of blood.
•Electrocardiogram.
•Chest X-ray, if medically indicated.
•X-ray of: the anteroposterior (AP) view of the pelvis; an AP view of the hip performed in 20° of internal rotation for templating; and a lateral view of the hip. At some centres, a shoot-through lateral view of the hip is also taken.
Other investigations:
•Lateral C-spine flexion and extension views for patients with rheumatoid arthritis affecting C-spine stability.
•Spirometry for patients with reduced pulmonary function.
•Cardiac assessment – echocardiography.
•Vascular assessment in patients with vascular compromise.
Informed consent
The procedure should be explained to the patient, along with all the risks of surgery. These are described later in the section on complications.
Cemented femoral component design
In the early days of THR, femoral prostheses were made out of cast stainless steel. This was not strong enough to sustain prolonged physiological loading and incidences of stem fracture led to development of cold-forged implants.
Titanium stems in cement transfer more load to the cement as the titanium is less stiff, leading to early cement fatigue and failure. Hence, cemented femoral components are made of stiffer materials – cobalt chrome or stainless steel.
A broad medial border on the prosthesis reduces the load on the cement. Hence, the diamond-shaped Muller prosthesis, which had a narrow medial border, is no longer used. The Thompson prosthesis used in hemiarthroplasty is also diamond-shaped in cross-section and has a narrow medial border. Femoral components should have a broad medial border to reduce cement strain, and a broader lateral border (e.g., C stem) to load the cement in compression (Figure 1.1).
Tapered stems (e.g., the Exeter system) help to transfer the load to cement evenly. Cement is stronger in compression. The flanged Charnley stem is broader laterally and helps to load the cement in compression. The C stem (DePuy) is thicker laterally and thinner medially – known as the third taper – which loads the medial cement mantle.
Offset
The offset of the stem is the perpendicular distance between the centre of the prosthetic femoral head and the longitudinal axis of the femoral stem (Figure 1.2). A high offset produces higher stress in the femoral stem and can lead to failure of the cement or metal. The advantage of a high offset, however, is that less force is required by the abductors because of an elongated lever arm. The offset of the prosthesis selected should normally reproduce the original offset of the patient.
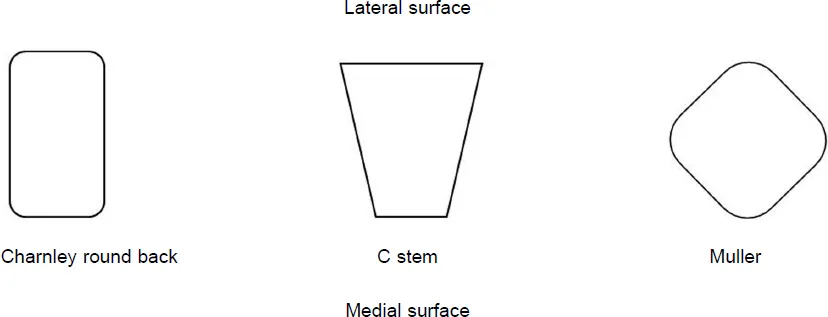
Figure 1.1. Diagrammatic cross-section of femoral stems to illustrate differences in design.
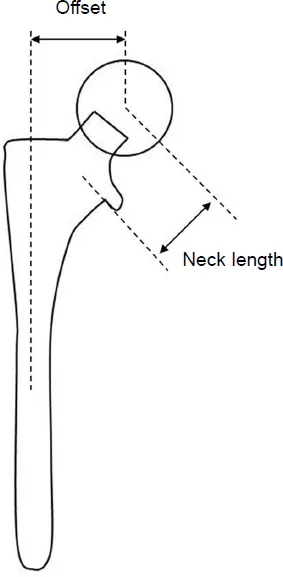
Figure 1.2. The offset and neck length of femoral components.
Most femoral prostheses have a high-offset option. For instance, the Charnley stem provides an offset of 40 or 45mm. In systems in which a range of stem sizes are available, the offset increases with increasing stem size. Increasing the neck length also results in a higher offset.
Implanting a femoral stem in varus alignment increases the offset. However, this is disadvantageous in cemented stems as it leads to an inadequate cement mantle in zones 3 and 7 and may lead to early failure. A cementless stem implanted in varus will be undersized and have less contact with the endosteum.
Offset can be altered during surgery by the following:
•Using a high-offset stem – this will increase offset without increasing leg length.
•Using a longer neck length – this will add to offset as well as leg length.
•Using an offset liner with a cementless socket. The centre of rotation is more laterally placed in offset compared to standard liners.
•Lateral placement of the acetabular component...
Table of contents
- Cover Page
- Title Page
- Copyright Page
- Contents
- Contributors
- Foreword
- Abbreviations
- Chapter 1: Arthroplasty
- Chapter 2: Shoulder disorders
- Chapter 3: Sports medicine
- Chapter 4: Spine and nerve injuries
- Chapter 5: Foot and ankle
- Chapter 6: Hand
- Chapter 7: Bone and soft tissue tumours
- Chapter 8: Infections
- Chapter 9: Non-union
- Chapter 10: Inflammatory joint disorders
- Chapter 11: Arthrodesis and amputations
- Chapter 12: Disorders in children
- Chapter 13: Trauma
- Chapter 14: Nerve injuries and neuromuscular disorders
- Chapter 15: Imaging
- Chapter 16: Clinical examination
- Chapter 17: Surgical approaches
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Current Orthopaedic Practice by Agarwal, Sanjeev in PDF and/or ePUB format, as well as other popular books in Medicine & Medical Theory, Practice & Reference. We have over 1.5 million books available in our catalogue for you to explore.