Medical students and junior doctors are an integral part of the healthcare system. On an academic gastroenterology service, they often initially evaluate the patients that are then staffed by the consulting physician. Like all clinical specialties, the acquisition of medical knowledge is required to gain expertise. There are several resources such as textbooks and evidence-based articles that are available for this purpose. Inspired from patient care, this book offers a fresh approach to clinical teaching. 50 Gastrointestinal Cases and Associated Imaging is a different kind of book. It encompasses a gamut of cases for which gastroenterologists are commonly consulted for in the hospital and outpatient setting. Each case is presented from initial history and workup including imaging (various modalities including endoscopy), followed by a brief discussion on management. Questions are presented to the reader in each case followed by an answer. Since each case is unique, the pertinent teaching points are tested in a question format within the case narrative. Similar to real-life scenarios, this helps the reader to retain the most important information. Why buy this book? Unlike listing facts as most review books do, teaching points are integrated into realistic clinical cases. Medical students to residents/registrars in internal medicine, emergency medicine, GI medicine, radiology and surgery would benefit from this book alike. Secondary audiences will include nurses and general practitioners who want to understand the presentation of common GI cases and associated imaging. Moreover, it could also be potentially used as a training tool – a valuable educational resource for senior colleagues who enjoy teaching. Finally, this book would make an excellent prerequisite prior to starting any gastroenterology rotation.
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineCase 1
A 44-year-old woman presents to the emergency room with right upper quadrant pain. The pain began about 20 minutes after eating dinner. It is described as a "shooting pain" that is constant, radiates to her back, and is 6/10 in intensity. The pain is worse on deep inspiration, and a tablet of oxycodone offers some relief. She denies nausea or vomiting. Her bowel movements are regular. She has never had this pain before.
What is your differential diagnosis?
The differential diagnosis includes cholelithiasis, acute cholecystitis, pancreatitis, gastritis, peptic ulcer disease, gastric volvulus, and intussusception.
Physical examination
| Vitals | Afebrile, HR 88 bpm, BP 130/78mmHg, oxygen saturation 99% on RA. |
| GEN | No distress. |
| HEENT | No scleral icterus. |
| CVS | Normal S1, S2. No murmurs, rubs, or gallops. |
| RESP | Clear to auscultation. |
| ABD | Soft and non-tender. No rigidity, guarding, or rebound tenderness. Bowel sounds are normal. Rectal examination reveals an empty vault. |
| EXT | No edema. |
Does this narrow your differential diagnosis?
Yes. Volvulus and intussusception can be removed from the differential diagnosis, as bowel sounds are altered in these clinical settings.
What blood test(s) will you order?
| LFTs | AST | 267 units/L |
| ALT | 285 units/L | |
| Alkaline phosphatase | 262 units/L | |
| Total bilirubin | 3.6mg/dL |
What is the pattern of the elevated LFTs?
Elevated LFTs usually suggest either a hepatocellular process or an obstructive (or cholestatic) process. A cholestatic process presents with elevated alkaline phosphatase and elevated total bilirubin levels. With the passage of a gallstone through the common bile duct, ALT may be the first measure to appear abnormal.
What other blood tests will you order?
CBC, CHEM-7, and bHCG.
All are within normal limits.
What imaging test will you order?
Your differential diagnosis already includes gallbladder pathology. Therefore, an ultrasound is the most important imaging test. The probe is placed over the ninth rib costal margin in the right mid-clavicular line. You see the image shown in Figure 1.

Figure 1.
Describe what you see and read on
The ultrasound shows a gallbladder in the sagittal view. Gallstones (white arrows) cast dark shadows (yellow arrows) on ultrasound. Changing the patient’s position demonstrates the stones are mobile. This image does not show a thickened gallbladder wall, or a black rim around the gallbladder wall suggesting fluid (pericholecystic fluid). The patient’s Murphy’s sign was negative on physical examination.
By now you have admitted the patient, kept her nil by mouth, started IV fluids, and called for a surgical consultation. Later you receive the radiology report and notice the patient’s common bile duct is 8mm.
What is your initial diagnosis, and how will you proceed?
The diameter of the common bile duct, measured in millimeters, should be less than or equal to the patient’s age in decades. So for this 44-year-old patient, who is in her fifth decade, it should be 5mm or less. An 8mm bile duct is suggestive, but not diagnostic, of at least some degree of biliary obstruction, and liver enzymes elevated in an obstructive pattern support this diagnosis. Given the numerous gallstones seen on ultrasound, a working diagnosis of choledocholithiasis – common duct stone(s) – is reasonable.
The next step is to obtain a GI consultation for a possible ERCP. This is arranged for the next day. The image shown in Figure 2 is obtained during the procedure.

Figure 2.
Describe what you see and read on
A fluoroscopic scout view of the right upper quadrant is obtained prior to the endoscopic procedure. Numerous stones are present in the gallbladder (black arrow). In addition, a solitary stone is seen outside the expected location of the gallbladder (white arrow), suggesting a stone in the biliary tree. A fluoroscopic image is obtained during the ERCP (Figure 3).
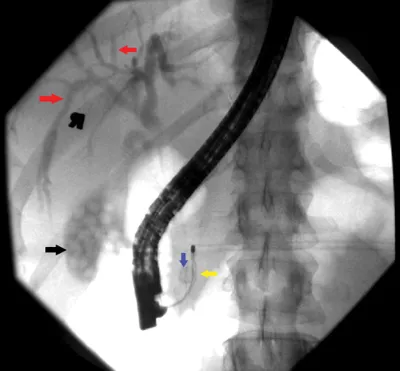
Figure 3.
Describe what you see and read on
This fluoroscopic image shows that the gallbladder (black arrow) and intrahepatic biliary ducts (red arrows) have been opacified with contrast. There is air in the common bile duct after biliary sphincterotomy, and a Dormia basket (yellow arrow) has engaged the stone (blue arrow) and is being used for its extraction.
A stone that was not seen on ultrasound was obstructing the common bile duct. This also explains why the patient had elevated LFTs, as the stone was causing biliary obstruction.
Overnight, the patient’s laboratory results improved. She remained pain-free and was discharged with a plan to have a laparoscopic cholecystectomy at a later date.
Clinical pearl
| • | Only two-thirds of common duct stones are seen on ultrasound when the common bile duct is less than 10mm. In this case the ultrasound did not show the stone in the duct, but there was a high clinical suspicion based on clinical history, elevated LFTs, and the slightly dilated common bile duct at 8mm. |
Impress your attending
What are gallstones made from?
Most gallstones (approximately 85%) are composed of cholestero...
Table of contents
- Cover Page
- Title Page
- Copyright Page
- Contents
- Foreword
- Abbreviations
- Case 1
- Case 2
- Case 3
- Case 4
- Case 5
- Case 6
- Case 7
- Case 8
- Case 9
- Case 10
- Case 11
- Case 12
- Case 13
- Case 14
- Case 15
- Case 16
- Case 17
- Case 18
- Case 19
- Case 20
- Case 21
- Case 22
- Case 23
- Case 24
- Case 25
- Case 26
- Case 27
- Case 28
- Case 29
- Case 30
- Case 31
- Case 32
- Case 33
- Case 34
- Case 35
- Case 36
- Case 37
- Case 38
- Case 39
- Case 40
- Case 41
- Case 42
- Case 43
- Case 44
- Case 45
- Case 46
- Case 47
- Case 48
- Case 49
- Case 50
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access 50 Gastrointestinal Cases and Associated Imaging by Shaikh, Abdullah A.,Hussain, Syed M.,Desilets, David J.,Catanzano, Tara M. in PDF and/or ePUB format, as well as other popular books in Medicine & Medical Theory, Practice & Reference. We have over 1.5 million books available in our catalogue for you to explore.