- 232 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Managing Money for General Practitioners, Second Edition
About this book
Now thoroughly revised and updated, the new edition of this popular book ensures that GPs and practice managers alike have a practical guide to the financial issues affecting medical practice. Although GPs delegate many of their management and administration functions to practice managers and other highly qualified staff, it is crucial for them to remain aware of how they are paid, how their income is taxed, how their tax will be settled, and the numerous financial problems that can arise in partnerships. Sound financial management is vital if these pitfalls are to be avoided. Written by specialists in the increasingly complex area of practice finance, this is an accessible guide for non-specialists, providing answers to routine queries and illustrating typical situations with worked examples.
Trusted by 375,005 students
Access to over 1 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
Personal FinanceCHAPTER 1 The legal framework of a medical practice
DOI: 10.1201/9781908911759-1
The National Health Service (NHS) was born in 1948. Since then there have been many changes, with a major reorganisation in 1990. A new general practitioner (GP) contract was introduced and, together with earlier changes from 1966, has been the basis of a medical practice’s income and its working practice. Radical proposals were introduced on 1 April 2004 based on protracted negotiations from October 2001, which were based on findings from a survey of GPs. The proposals endeavoured to rectify many of the findings brought to light, such as low morale, high worldoads, and dissatisfaction with pay and conditions.
The Department of Health (DoH) was set up to support the government to improve healthcare, set standards and secure resources to deliver services to the country. To help achieve their aims, strategic health authorities (SHAs) were set up in April 2002.
SHAs have the role of developing strategies for the NHS and ensuring that local NHS organisations deliver services well. To achieve this, primary care trusts (PCTs) were created, with the responsibility of managing healthcare in a local area.
PCTs are statutory bodies that receive 75% of the NHS budget, and liaise with local authorities and other agencies to provide health needs at the primary and secondary levels. Being local, their role is to assess local needs based on their knowledge, and plan accordingly. PCTs have autonomy and much responsibility. Their powers are far reaching and include commissioning of services and purchase of property.
Primary care is provided by GPs, dentists, opticians, pharmacists and, more recently, walk-in centres, which provide instant access to advice and treatment. Secondary care is provided through acute, ambulance, care and mental health trusts. Most patients will be referred to secondary care by their GP, although in certain situations GPs can provide secondary care, e.g. counselling.
Figure 1.1 summarises all of the above.
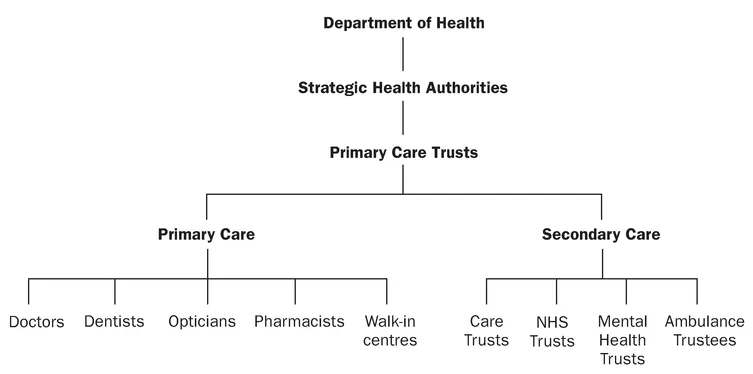
Figure 1.1 The organisation of the health service.
THE MEDICAL PRACTICE
General practitioners provide primary care, with the power to refer to secondary care. Their role is to provide healthcare in a designated local area and provide basic advice and treatment. They can also provide education to encourage preventative medicine, give vaccinations and carry out simple surgical operations.
To fund the practice, GPs receive income from the PCT, the amount depending on whether they provide general medical services (GMS) or personal medical services (PMS). Funding is discussed in Chapter 5. Changes to the GMS contract were introduced in April 2004, and the financial bible is now the Statement of Financial Entitlements (SFE), which replaces the familiar ‘Red Book’ that has adorned GPs’ bookshelves for over 40 years. The SFE sets out the guidance relating to payments made by a PCT to a contractor under a GMS contract. Copies of the document are available from the DoFF website www.dh.gov.uk.
GENERAL PRACTITIONER Status
GPs are unique as independent contractors to the NHS. GPs are treated as selfemployed individuals who pay their own tax and national insurance liabilities. They are responsible for organising and paying for their surgery, staff and other overheads. However, as far as their income is concerned, they have limited control and, as will be seen later in this book, the generation of income is on a very different footing to that of other self-employed professionals.
Although generally self-employed, the GP is entitled to be a member of the NHS Pension Scheme - an occupational scheme for employees. Full details of this scheme are discussed in Chapter 10, but suffice to say at this stage that although GPs pay between 5% and 8.5% of their superannuable earnings into their scheme, the employer, i.e. the PCT, is responsible for a further 14%. Other self-employed persons do not have this attractive advantage.
Great care must be taken to ensure that the correct status is awarded to a doctor. The recent changes to both PMS and GMS contracts have encouraged many doctors to become salaried partners or doctors. This category of doctor is rarely self-employed, and professional advice should be sought to ensure that the GP obtains the status best suited to their individual circumstances.
CHAPTER 2 The structure of medical practice
DOI: 10.1201/9781908911759-2
The business structure of general practice has been run along traditional lines since the inception of the NHS in 1948. Practices have been run by the partners who have actually performed most of the clinical work. This structure was encouraged by the old ‘Red Book’ rules, particularly the calculation of the basic practice allowance and the restriction on GP Principal numbers imposed by the Medical Practices Committee. Thus, prior to the new contract only the minority of the workforce was made up of salaried doctors, registrars, assistants or locums.
The new contract changes all this, and many commentators refer to the key issue of the new contract as being skills-mix. It is now entirely up to individual practices how they structure both the business management and medical workforce within their walls. Indeed, it is no longer necessary to replace a retiring partner with an identical substitute in order to maintain practice income. It is financially favourable to restrict the number of profit-sharing partners to maximise individual shares and to employ salaried doctors or other healthcare individuals to help provide medical care.
In the current climate, when an existing partner retires the continuing partners can take the opportunity to consider whether the outgoing partner should be replaced by a different healthcare professional who will bring alternative skills to the practice. They also look to achieve list sizes that provide for optimum use of existing partners. Practices are therefore striving to achieve the ideal practice structure with a view to maximising profits. The new contract has made medical practice more of a business than a salaried service, with the partners effectively acting as shareholders. While the common mission statement of a practice might be ‘to provide the highest quality of medical care’, there will always be the tacit aim of maximising profit alongside. It is no longer good enough simply to expect money to flow in for being a good doctor, as such a policy always produces a mediocre financial reward. To achieve above-average rewards, GPs have to be prepared for change, willing to embrace new opportunities and positive in setting up the right systems.
The ideal structure of the practice will be dictated by several factors, such as:
- the availability of doctors in the area
- the partners’ preferences for providing management/specialisation/out of hours
- the skills of other employed staff
- the management culture
- opportunities for work outside the practice
- competition with other local providers
- the demographics of the local population.
Opportunities to change a practice’s structure may occur only when an existing partner retires or resigns. In the meantime, practices need to consider changing the practice list size in order to change the balance of staff and partners. Alternatively, practices can consider merging or splitting partnerships, particularly when recruitment of partners is a major difficulty.
There are, of course, other issues that need to be considered when attempting to formulate the ideal practice structure. These include the following.
- Should the practice diversify into non-GMS/PMS activities?
- Should the practice appoint a specialist firm of accountants, or indeed a management consultant?
- Should the practice change its information technology systems to ensure that the system is capable of recording quality data, retrieving quality data and dealing with electronic claims?
Given that the ideal practice structure is geared to maximise earnings, it is worth knowing the common features of both high and low earners. In conducting their annual survey into the accounts of their GP clients, Association of Independent Specialist Medical Accountants (AISMA) members have been able to identify, on a regular basis, the features that determine whether practices are high earners or low earners. High earners have the following features:
- stable partnership (low turnover of partners)
- partners work as a team, trust each other, plan ahead and meet regularly
- top-rate databases on patients and treatments
- partners have similar philosophies in terms of the dichotomy between money and patient care
- proactive rather than reactive teams
- good managers of time
- well-organised GPs with strong staff teams and good skills-mix among them
- GPs who delegate well to nurses, health visitors, etc.
- GPs who work long hours, have low deputising costs and a high level of non-NHS earnings
- GPs with very high list sizes (normally single-handed GPs)
- GPs who have the ability to dispense
- PMS GPs who have taken advantage of growth funding and freed up time to perform more lucrative tasks
- GPs who are heavily involved with their primary care organisation (PCO)
- GPs with the most competent and skilled practice managers and specialist accountants
- GPs who were early fundholders.
In fact, these features could well represent a guide to those GPs earning the most. Practices should score themselves out of 10 for each of the 15 items above – a total of 125 or more means a good performance, a score of 100-plus is average, and a score of less than 100 means that practices have work to do on the practice, not in the practice, to increase earnings significantly.
The features of the low-earning practices who, under the new contract, could expect financial disaster to befall are:
- practices involved in partnership disputes
- GPs with inadequate resources, such as staff, equipment and space (such GPs often have the wrong staff-mix or have a loyal contingent of staff who have been promoted over the years but do not necessarily have the relevant skills)
- badly organised practices that typically have an excessive number of patients; poor internal control systems are a feature of such practices
- GPs who are bad managers of time
- GPs who work as individuals and not as a team, who gave little or no thought to fundholding or an early entrance into P...
Table of contents
- Cover
- Half Title
- Title
- Copyright
- Contents
- Preface to the second edition
- About the editor
- Contributors
- Acknowledgements
- Introduction
- 1 The legal framework of a medical practice
- 2 The structure of medical practice
- 3 Partnership agreements
- 4 Practice accounts
- 5 The contract for services
- 6 Partners’ funds and financing the practice
- 7 Other sources of income
- 8 Practice expenditure
- 9 Practice premises
- 10 NHS Pension Scheme
- 11 Pensions and personal financial planning
- 12 Forward planning
- 13 The taxation of earnings
- 14 Capital taxation
- 15 VAT and the GP
- 16 A compilation of financial tit-bits
- 17 Financial horror stories
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Managing Money for General Practitioners, Second Edition by Mike Gilbert in PDF and/or ePUB format, as well as other popular books in Medicine & Personal Finance. We have over one million books available in our catalogue for you to explore.