"Immediate loading meets digital treatment planning in this latest implant title. The authors emphasize that the preservation of alveolar hard and soft tissues using the immediacy concept is more predictable than is the reconstruction of the hard and soft tissues using the traditional delayed approach once resorption has occurred. Immediate loading has also shown to be very predictable in cases of full-arch reconstructions and has become the treatment of choice in cases where appropriate criteria are met. Because a thorough understanding of analog protocols is necessary before attempting a digital case, the authors review these fundamental concepts to provide context for the transition to the digital realm. The book begins by outlining the principles of immediate loading and those of digital workflows before delving into individual clinical situations ranging from single teeth to full arches, both with and without bone resorption. Information on prosthetics is included as well as surgical treatment planning. The book concludes with a chapter entirely devoted to case presentations of all the treatment types covered throughout. If you are ready to step into the future of dental implant treatment, this book is for you!"

eBook - ePub
The Immediacy Concept
Treatment Planning from Analog to Digital
- 404 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
The Immediacy Concept
Treatment Planning from Analog to Digital
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
SECTION V
ZYGOMATIC IMPLANTS
Included topics:
- Biomechanical Principles for Zygomatic Implants
- New Zygomatic Implant Design
- Prevention and Management of Zygomatic Implant Complications
17
Biomechanical Principles for Zygomatic Implants
Edmond Bedrossian, DDS
The zygomatic implant has been used in the treatment of the edentulous maxilla for almost three decades.1 This chapter intends to consolidate the information described in the literature with regard to the biomechanical principles of the zygomatic implant under load, the trajectory of the zygomatic implant, the use of the zones of the maxilla, as well as the zygomatic anatomy guided approach (ZAGA) for treatment planning this group of patients. The use of the new redesigned round and flat implants will also be described.
The positions of the maxillary sinus and the nasal aperture as well as the superior, medial, and posterior resorption pattern of the edentulous maxilla may limit the vertical as well as the horizontal bone volume necessary to house endosseous implants within the alveolar housing for fabrication of a fixed implant-supported prosthesis.
Various grafting procedures to reconstruct bone volume in the edentulous maxilla have been reported in the literature by multiple authors.1–5 Keller et al and Tollman have reported 87% and 95% implant and prosthetic success rates respectively with grafting of the maxilla with delayed implant placement and delayed loading.6,7 Autogenous onlay and/or Le Fort I procedures have success rates of 80% and 77% for grafting with delayed implant placement and for grafting with simultaneous implant placement respectively as reported by Rasmusson et al.8 Extended treatment time, inability to wear a functional provisional prosthesis during the various healing times, and the morbidity associated with the various stages of the treatment are factors that limit the number of patients who choose to have reconstruction of their maxillae.
The contemporary literature has described the use of tilted implants to avoid extensive bone grafting procedures for patients who have residual alveolar bone in the anterior maxilla and the premolar region.9–11 To determine the appropriate type of surgical protocol for patients, the understanding of the zones of the maxilla is a rapid screening process that enables communication between the implant team (Fig 17-1). In order to place tilted implants for posterior support, bone must be present in zone 1 (the anterior maxilla) and zone 2 (the premolar region).
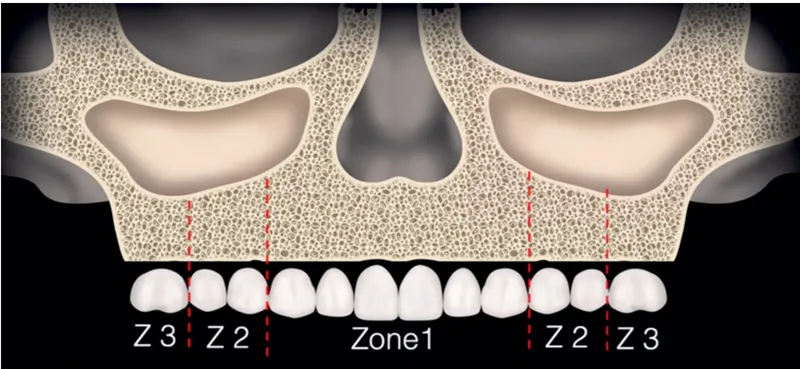
FIG 17-1 Zones of the maxilla. (Copyright E. M. Titcomb 2022.)
However, for patients who have alveolar bone in zone 1 but are lacking alveolar bone height in zones 2 and 3, the zygomatic implant is considered to establish posterior support and to avoid bone grafting procedures. Over the last three decades, the use of the zygomatic implant has been studied internationally, with reported success rates between 94% and 100%.12–17 The zygomatic implant engages the limited crestal alveolar bone of the residual maxilla in the second premolar to first molar region at its platform and the zygomatic bone at its apex, allowing for a quad-cortical stabilization of the zygomatic implant.
Delayed as well as immediate loading of the implants has also been reported in the literature. Delayed loading of zygomatic implants was reported by Prof Brånemark in 2004 with a cumulative survival rate (CSR) of 94%.16 Bedrossian reported on the 7-year prospective follow-up of patients treated using the immediate-load protocol with a CSR of 97.2%.18 In 2014, Aparicio et al published a 10-year prospective study using the immediate-load protocol with a similar 97.71% CSR.19
The author would like to emphasize that the placement of the zygomatic implant is an advanced procedure. A systematic pretreatment evaluation method,20 as well as comprehensive appreciation for the surgical anatomy and the prosthetic biomechanical principles by the implant team, is imperative for favorable outcomes.
The Zygomatic Implant Under Function
In 2007, Ujigawa and colleagues21 described the weight-bearing bone associated with the use of the zygomatic implant. In their finite element analysis (FEA) study, they reported that the zygomatic bone, and not the maxilla alveolus, was primarily responsible for the support of the simulated occlusal loads (Fig 17-2). In 2013 and 2015, Freedman et al22,23 corrected the observation in the Ujigawa study. Freedman et al explained that the highlighted area over the lateral cortex of the zygoma reported as the load-bearing area in the Ujigawa article was in fact the origin of the masseter muscle, which was highlighted under activation. Therefore, it did not represent the zygomatic bone as being the primary weight-bearing bone when the zygomatic implant is under load by the attached fixed prosthesis. Freedman et al reported that the maxillary crest is the primary support and plays a major role in the distribution of the occlusal loads and that the preservation and the anchoring of the implant platform at the maxillary crest is advantageous.
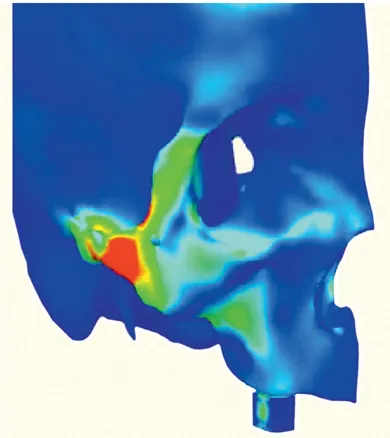
FIG 17-2 The origin of the masseter muscle is highlighted in red. (Reprinted with permission from Ujigawa et al.21)
There has been momentum by some authors to recommend the extrasinus technique, a modification to the ad modum Brånemark protocol for the placement of all zygomatic implants. The extrasinus or extramaxillary technique includes intentional removal of the maxillary crestal alveolar bone. Although this technique may be considered easier than the traditional technique, the intentional removal of the maxillary crestal bone cannot be justified. To support this statement, in 2015, Freedman et al addressed the extrasinus placement of the zygomatic implant.23 In this new FEA, the first model had two zygomatic implants placed in an extrasinus position, with the implant platforms supported by the maxillary crestal bone. The implants were connected together by a rigid cross-arch splinted partial denture. The second model was the duplication of the first model, but the area of the maxillary alveolar bone supporting the implant platform was removed, which is an inherent consequence of the described “extrasinus implant placement” technique (Fig 17-3a). In both mode...
Table of contents
- Cover
- Half Title Page
- Copyright page
- Title page
- Contents
- Foreword
- Preface
- Contributors
- SECTION I The Immediacy Concept
- SECTION II The Digital Workflow
- SECTION III Treating Fully Edentulous Arches
- SECTION IV Prosthetics for Full-Arch Rehabilitation
- SECTION V Zygomatic Implants
- Index
- Back Cover
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access The Immediacy Concept by Edmond Bedrossian,E. Armand Bedrossian,Lawrence Brecht in PDF and/or ePUB format, as well as other popular books in Medicine & Dentistry. We have over 1.5 million books available in our catalogue for you to explore.