Edmond Bedrossian, E. Armand Bedrossian, Lawrence Brecht
This is a test
This is a test
Buch teilen
404 Seiten
English
ePUB (handyfreundlich)
Über iOS und Android verfügbar
eBook - ePub
The Immediacy Concept
Treatment Planning from Analog to Digital
Edmond Bedrossian, E. Armand Bedrossian, Lawrence Brecht
Angaben zum Buch
Buchvorschau
Inhaltsverzeichnis
Quellenangaben
Über dieses Buch
"Immediate loading meets digital treatment planning in this latest implant title. The authors emphasize that the preservation of alveolar hard and soft tissues using the immediacy concept is more predictable than is the reconstruction of the hard and soft tissues using the traditional delayed approach once resorption has occurred. Immediate loading has also shown to be very predictable in cases of full-arch reconstructions and has become the treatment of choice in cases where appropriate criteria are met. Because a thorough understanding of analog protocols is necessary before attempting a digital case, the authors review these fundamental concepts to provide context for the transition to the digital realm. The book begins by outlining the principles of immediate loading and those of digital workflows before delving into individual clinical situations ranging from single teeth to full arches, both with and without bone resorption. Information on prosthetics is included as well as surgical treatment planning. The book concludes with a chapter entirely devoted to case presentations of all the treatment types covered throughout. If you are ready to step into the future of dental implant treatment, this book is for you!"
Häufig gestellte Fragen
Wie kann ich mein Abo kündigen?
Gehe einfach zum Kontobereich in den Einstellungen und klicke auf „Abo kündigen“ – ganz einfach. Nachdem du gekündigt hast, bleibt deine Mitgliedschaft für den verbleibenden Abozeitraum, den du bereits bezahlt hast, aktiv. Mehr Informationen hier.
(Wie) Kann ich Bücher herunterladen?
Derzeit stehen all unsere auf Mobilgeräte reagierenden ePub-Bücher zum Download über die App zur Verfügung. Die meisten unserer PDFs stehen ebenfalls zum Download bereit; wir arbeiten daran, auch die übrigen PDFs zum Download anzubieten, bei denen dies aktuell noch nicht möglich ist. Weitere Informationen hier.
Welcher Unterschied besteht bei den Preisen zwischen den Aboplänen?
Mit beiden Aboplänen erhältst du vollen Zugang zur Bibliothek und allen Funktionen von Perlego. Die einzigen Unterschiede bestehen im Preis und dem Abozeitraum: Mit dem Jahresabo sparst du auf 12 Monate gerechnet im Vergleich zum Monatsabo rund 30 %.
Was ist Perlego?
Wir sind ein Online-Abodienst für Lehrbücher, bei dem du für weniger als den Preis eines einzelnen Buches pro Monat Zugang zu einer ganzen Online-Bibliothek erhältst. Mit über 1 Million Büchern zu über 1.000 verschiedenen Themen haben wir bestimmt alles, was du brauchst! Weitere Informationen hier.
Unterstützt Perlego Text-zu-Sprache?
Achte auf das Symbol zum Vorlesen in deinem nächsten Buch, um zu sehen, ob du es dir auch anhören kannst. Bei diesem Tool wird dir Text laut vorgelesen, wobei der Text beim Vorlesen auch grafisch hervorgehoben wird. Du kannst das Vorlesen jederzeit anhalten, beschleunigen und verlangsamen. Weitere Informationen hier.
Ist The Immediacy Concept als Online-PDF/ePub verfügbar?
Ja, du hast Zugang zu The Immediacy Concept von Edmond Bedrossian, E. Armand Bedrossian, Lawrence Brecht im PDF- und/oder ePub-Format sowie zu anderen beliebten Büchern aus Medicine & Dentistry. Aus unserem Katalog stehen dir über 1 Million Bücher zur Verfügung.
Prevention and Management of Zygomatic Implant Complications
17
Biomechanical Principles for Zygomatic Implants
Edmond Bedrossian, DDS
The zygomatic implant has been used in the treatment of the edentulous maxilla for almost three decades.1 This chapter intends to consolidate the information described in the literature with regard to the biomechanical principles of the zygomatic implant under load, the trajectory of the zygomatic implant, the use of the zones of the maxilla, as well as the zygomatic anatomy guided approach (ZAGA) for treatment planning this group of patients. The use of the new redesigned round and flat implants will also be described.
The positions of the maxillary sinus and the nasal aperture as well as the superior, medial, and posterior resorption pattern of the edentulous maxilla may limit the vertical as well as the horizontal bone volume necessary to house endosseous implants within the alveolar housing for fabrication of a fixed implant-supported prosthesis.
Various grafting procedures to reconstruct bone volume in the edentulous maxilla have been reported in the literature by multiple authors.1–5 Keller et al and Tollman have reported 87% and 95% implant and prosthetic success rates respectively with grafting of the maxilla with delayed implant placement and delayed loading.6,7 Autogenous onlay and/or Le Fort I procedures have success rates of 80% and 77% for grafting with delayed implant placement and for grafting with simultaneous implant placement respectively as reported by Rasmusson et al.8 Extended treatment time, inability to wear a functional provisional prosthesis during the various healing times, and the morbidity associated with the various stages of the treatment are factors that limit the number of patients who choose to have reconstruction of their maxillae.
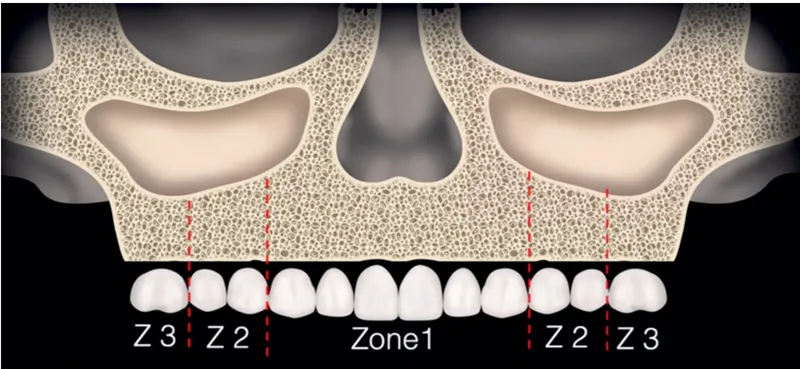
The contemporary literature has described the use of tilted implants to avoid extensive bone grafting procedures for patients who have residual alveolar bone in the anterior maxilla and the premolar region.9–11 To determine the appropriate type of surgical protocol for patients, the understanding of the zones of the maxilla is a rapid screening process that enables communication between the implant team (Fig 17-1). In order to place tilted implants for posterior support, bone must be present in zone 1 (the anterior maxilla) and zone 2 (the premolar region).
FIG 17-1 Zones of the maxilla. (Copyright E. M. Titcomb 2022.)
However, for patients who have alveolar bone in zone 1 but are lacking alveolar bone height in zones 2 and 3, the zygomatic implant is considered to establish posterior support and to avoid bone grafting procedures. Over the last three decades, the use of the zygomatic implant has been studied internationally, with reported success rates between 94% and 100%.12–17 The zygomatic implant engages the limited crestal alveolar bone of the residual maxilla in the second premolar to first molar region at its platform and the zygomatic bone at its apex, allowing for a quad-cortical stabilization of the zygomatic implant.
Delayed as well as immediate loading of the implants has also been reported in the literature. Delayed loading of zygomatic implants was reported by Prof Brånemark in 2004 with a cumulative survival rate (CSR) of 94%.16 Bedrossian reported on the 7-year prospective follow-up of patients treated using the immediate-load protocol with a CSR of 97.2%.18 In 2014, Aparicio et al published a 10-year prospective study using the immediate-load protocol with a similar 97.71% CSR.19
The author would like to emphasize that the placement of the zygomatic implant is an advanced procedure. A systematic pretreatment evaluation method,20 as well as comprehensive appreciation for the surgical anatomy and the prosthetic biomechanical principles by the implant team, is imperative for favorable outcomes.
The Zygomatic Implant Under Function
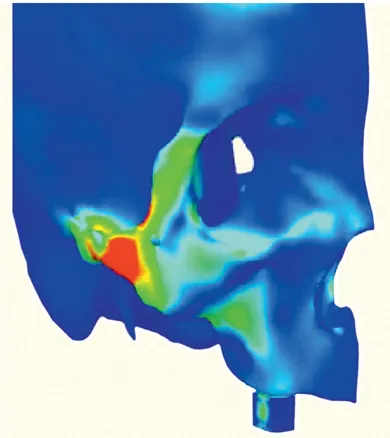
In 2007, Ujigawa and colleagues21 described the weight-bearing bone associated with the use of the zygomatic implant. In their finite element analysis (FEA) study, they reported that the zygomatic bone, and not the maxilla alveolus, was primarily responsible for the support of the simulated occlusal loads (Fig 17-2). In 2013 and 2015, Freedman et al22,23 corrected the observation in the Ujigawa study. Freedman et al explained that the highlighted area over the lateral cortex of the zygoma reported as the load-bearing area in the Ujigawa article was in fact the origin of the masseter muscle, which was highlighted under activation. Therefore, it did not represent the zygomatic bone as being the primary weight-bearing bone when the zygomatic implant is under load by the attached fixed prosthesis. Freedman et al reported that the maxillary crest is the primary support and plays a major role in the distribution of the occlusal loads and that the preservation and the anchoring of the implant platform at the maxillary crest is advantageous.
FIG 17-2 The origin of the masseter muscle is highlighted in red. (Reprinted with permission from Ujigawa et al.21)
There has been momentum by some authors to recommend the extrasinus technique, a modification to the ad modum Brånemark protocol for the placement of all zygomatic implants. The extrasinus or extramaxillary technique includes intentional removal of the maxillary crestal alveolar bone. Although this technique may be considered easier than the traditional technique, the intentional removal of the maxillary crestal bone cannot be justified. To support this statement, in 2015, Freedman et al addressed the extrasinus placement of the zygomatic implant.23 In this new FEA, the first model had two zygomatic implants placed in an extrasinus position, with the implant platforms supported by the maxillary crestal bone. The implants were connected together by a rigid cross-arch splinted partial denture. The second model was the duplication of the first model, but the area of the maxillary alveolar bone supporting the implant platform was removed, which is an inherent consequence of the described “extrasinus implant placement” technique (Fig 17-3a). In both mode...