eBook - ePub
Epidemiology of Injury in Adventure and Extreme Sports
- 184 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Epidemiology of Injury in Adventure and Extreme Sports
About this book
This book reviews the existing data on the frequency and distribution of injuries and the factors contributing to injuries in adventure and extreme sports. Further, it suggests injury prevention strategies and provides recommendations for future research. Providing the first comprehensive compilation of epidemiological data over a range of new age sports considered to be adventurous and extreme, this publication is also the first of its kind to track down all of the major literature associated with the topic. A uniform and evidence-based approach to organizing and interpreting the literature is used in all chapters. All of the sport-specific chapters are laid out with the same basic headings making it easier for the reader to find common information across chapters. Sports physicians, physical therapists, recreation managers, researchers, injury prevention specialists, the adventure and extreme sport industry, and the adventure and extreme sport participants themselves will find the book useful in identifying problem areas in which appropriate preventive measures can be initiated to reduce the risk and severity of injuries. They will also want to use the book as a source for future research related to injuries in adventure and extreme sports.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineOcean and Freshwater Sports
Heggie TW, Caine DJ (eds): Epidemiology of Injury in Adventure and Extreme Sports.
Med Sport Sci. Basel, Karger, 2012, vol 58, pp 57–79
Med Sport Sci. Basel, Karger, 2012, vol 58, pp 57–79
______________________
The Epidemiology of Injury in Scuba Diving
Peter L. Buzzacott
School of Sports Science, Exercise and Health, University of Western Australia, Crawley, W.A., Australia
______________________
Abstract
The epidemiology of injury associated with recreational scuba diving is reviewed. A search of electronic databases and reference lists identified pertinent research. Barotrauma, decompression sickness and drowning-related injuries were the most common morbidities associated with recreational scuba diving. The prevalence of incidents ranged from 7 to 35 injuries per 10,000 divers and from 5 to 152 injuries per 100,000 dives. Recreational scuba diving fatalities account for 0.013% of all-cause mortality aged ≥15 years. Drowning was the most common cause of death. Among treated injuries, recovery was complete in the majority of cases. Dive injuries were associated with diver-specific factors such as insufficient training and preexisting medical conditions. Environmental factors included air temperature and flying after diving. Dive-specific factors included loss of buoyancy control, rapid ascent and repetitive deep diving. The most common event to precede drowning was running out of gas (compressed air). Though diving injuries are relatively rare prospective, longitudinal studies are needed to quantify the effects of known risk factors and, indeed, asymptomatic injuries (e.g. brain lesions). Dive injury health economics data also remains wanting. Meanwhile, health promotion initiatives should continue to reinforce adherence to established safe diving practices such as observing depth/time limits, safety stops and conservative ascent rates. However, there is an obvious lack of evaluated diving safety interventions.
Copyright © 2012 S. Karger AG, Basel
Ambient pressure increases by one atmosphere for each additional depth of 10 m of seawater. Laborers working underwater in caissons while building the Eads and Brooklyn Bridges breathed air at a pressure equivalent to the ambient pressure of the depth of the workplace and high enough to repel the surrounding water. Upon returning to the surface some would experience pain and adopt a posture reminiscent of a fashionable pose known as the ‘Grecian bend’. This affliction became known as ‘the bends’ [1]. A century ago, the Royal Navy commissioned J.S. Haldane and colleagues to produce a set of tables prescribing time limits for each depth a diver might safely work at while teams of sailors manned compressed-air pumps to force fresh air down against the pressure of the water. Then, during the Second World War, Jacques Cousteau and Émile Gagnan invented a dual-hose regulator which allowed divers to
carry compressed gas in cylinders and to inhale it at a pressure equivalent to that in which they were diving. The self-contained underwater breathing apparatus (scuba) had arrived. Since first appearing in the late 1940s as a recreational pursuit, scuba diving has grown steadily in popularity and, concurrently, so too has the incidence of diving-related injuries. This review considers the epidemiology of injury resulting from the adventure sport of recreational scuba diving, conventionally defined as no-stop diving with compressed gas in open water to depths of ≤40 m. Military, commercial, technical, rebreather, cave, occupational harvester and breath-hold diving are not considered here.
An electronic search was made of articles indexed by Allied and Complementary Medicine (AMED), Ovid Journals, CAB Abstracts, EMBASE, ERIC, Medline and PsychInfo using the search terms ‘div$ and (fatal$ or scuba or risk or injur$)’ and Google Scholar using the search terms ‘(diver OR diving) AND (fatal OR scuba OR risk OR injury)’. Publications were assessed for relevance to this review and either rejected, downloaded from electronic archives or acquired in hardcopy from libraries. Each publication's reference list was examined for additional potentially relevant publications and those identified were also similarly obtained. One limitation within the literature that soon became apparent was the lack of uniformity in reporting incidence and prevalence of diving injuries. In Leicester, for example, mortality incidence was given per 100,000 divers and yet divers may make any number of dives from 1 to 500 within a single year [2]. The Professional Association of Diving Instructors (PADI) cite a number of deaths over a 10-year period without stating how many member-years that period included [3] while other studies estimate the incident rate of decompression sickness (DCS) at either 1 case per number of dives or else by the number of cases per 100,000 dives. Rarely are incidence rates given per dives (or divers), per year.
Who Is Affected by Injury?
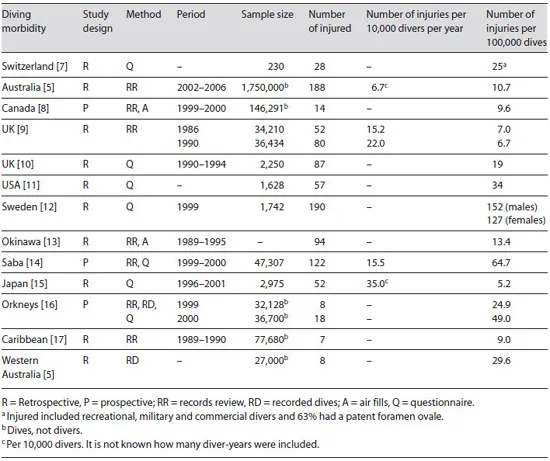
Between 1995 and 2007 3,558 divers were treated for decompression illness (DCI) in Australia [4]. During the first 3 years of running dive tours to the deliberately scuttled (former HMAS) Swan shipwreck offshore from the south-west of Australia, a single dive tour operator documented 27,000 dives and 8 known cases of DCI, an incident rate of 29.6 cases per 105 dives, almost three times higher than the Australia-wide estimate of 10.7 cases per 105 dives [5]. One potential reason why these rates differ may be that the lower figure includes many dives made well within the prescribed time/ depth limits while the higher figure may have resulted from divers maximizing their dive time on the shipwreck which, as Vann et al. [6] suggest in a recent review of DCS, would closer approximate the ‘true’ prevalence among dives made to the maximum limits. Diving morbidity studies identified during the literature search are summarized in table 1.
Table 1. Recreational diving morbidity studies
Where Does Injury Occur?
The protean nature of diving injuries means there is barely a location on or within the human body that is not susceptible to insult. The most common injury involves trauma to the ears and/or sinuses [18], which may not require treatment and often go unreported [19]. Of 49 confirmed cases of DCS reported to the Diver's Alert Network (DAN) in 2007, 6 (12%) included loss of bladder control and 23 (46%) included skin manifestations [19]. Of 347 medical inquiries to DAN concerning barotrauma, 212 (62%) affected the ear, 57 (16%) were related to the sinuses, 51 (15%) to the lungs, 21 (6%) to the face, 3 (1%) to the stomach, and 3 (1%) were related to the teeth [19]. Pressure-related injuries usually occur during descent or ascent. The genesis of DCS occurs at depth, where tissues take on additional dissolved inert gas, though physical injuries manifest following ascent when th...
Table of contents
- Cover Page
- Front Matter
- The Epidemiology of Injury in Adventure and Extreme Sports
- The Epidemiology of Injury in Mountaineering, Rock and Ice Climbing
- The Epidemiology of Injury in Hang-Gliding and Paragliding
- The Epidemiology of Injury in Scuba Diving
- The Epidemiology of Injury among Surfers, Kite Surfers and Personal Watercraft Riders: Wind and Waves
- The Epidemiology of Injury in Canoeing, Kayaking and Rafting
- The Epidemiology of Injury in Bungee Jumping, BASE Jumping, and Skydiving
- The Epidemiology of Extreme Hiking Injuries in Volcanic Environments
- The Epidemiology of Injury in Skateboarding
- The Epidemiology of Injury in ATV and Motocross Sports
- Author Index
- Subject Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Epidemiology of Injury in Adventure and Extreme Sports by T. W. Heggie,D. J. Caine,T.W., Heggie,D.J., Caine, D. J. Caine,A. P. Hills,T. Noakes,D.J., Caine,A.P., Hills,T., Noakes in PDF and/or ePUB format, as well as other popular books in Medicine & Emergency Medicine & Critical Care. We have over 1.5 million books available in our catalogue for you to explore.